이달의 증례
- 페이지 경로
- HOME > 자료실 > 이달의 증례



|
이달의 중재술 / 2017년 11월 Acute myocardial infarction due to coronary embolism, Is the cause only thrombi? |
|||||||
| 저자 | Presenter: 조성수 / Sungsoo Cho, MDOperator: 조성수 / Sungsoo Cho, MD | ||||||
|---|---|---|---|---|---|---|---|
| 소속 | Institution: 단국대학교 의과대학, 단국대학교병원 / Dankook University College of Medicine, Dankook University Hospital | ||||||
|
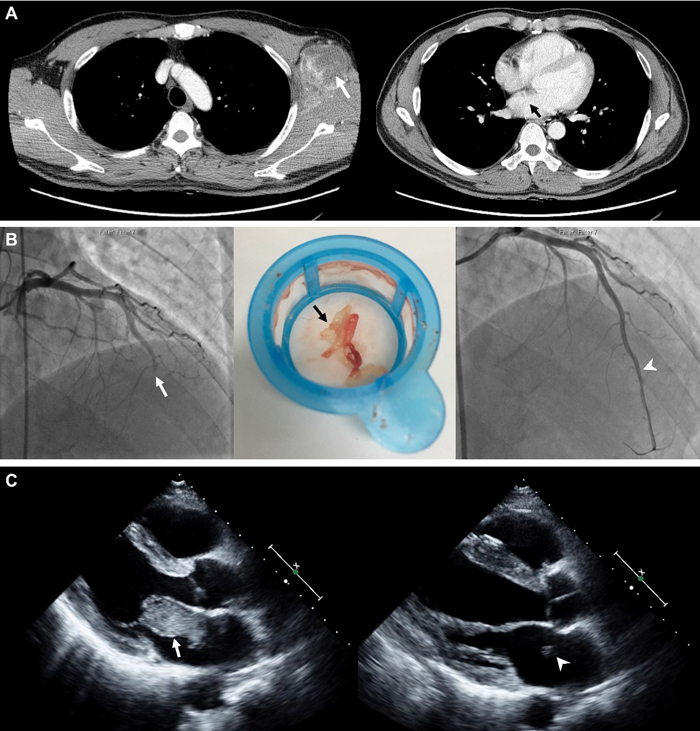
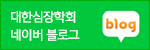
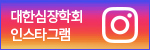
A 54-year old male visited emergency room (ER) for a sudden chest pain. In his previous medical history, he was diagnosed as left axillary undifferentiated pleomorphic sarcoma 2 years ago without metastasis in heart at our hospital (Figure 1A). Despite surgery, multiple sessions of chemotherapy and radiation therapy, the cancer proliferated. One year after diagnosis, he started taking pembrolizumab to target metastasis of sarcoma. After initiation of pembrolizumab, the patient was hospitalized for a sudden cardiac arrest due to AMI induced by embolus and angioplasty was performed at other hospital a year ago. In his electrocardiogram at ER, ST segment elevation was shown at V1-V5 lead. We performed coronary angiography and found a total occlusion of distal left anterior descending artery. By utilizing a thromboaspirate suction catheter, we suctioned the area multiple times and obtained the mucoid white tissue debris. In final coronary angiography, the coronary flow was completely restored (Figure 1B). In his echocardiography a year ago, a huge floating mass found in the left atrium. The mass was significantly decreased in size on new echocardiography (Figure 1C). The aspirated tissue was sent for examination to confirm the histology. A low-powered light-microscopic view showed several fibrinous thromboemboli (Figure 2A) that were composed of discohesive round sarcoma cells with frequent mitotic figures and scattered pleomorphic giant cells (Figure 2B). The tumor cells were diffusely immunoreactive with CD68, a macrophage marker, and vimentin, a representative mesenchymal marker. Also, we compared the cytologic and immunohistochemical findings of primary axillary sarcoma (Figure 2E and 2F) with the acquired intracoronary embolus tissue. We finally confirmed that intracoronary embolus tissue consists of metastatic sarcoma cells from primary axillary sarcoma tissue. Key words: Sarcoma, coronary embolus
|
|||||||
| 첨부파일1 | |||||||
| 첨부파일2 | |||||||

- Tel 02-3275-5258
- Fax 02-3275-5259
- E-mail herz1@circulation.or.kr
- Copyright© The Korean Society of Cardiology


- 심장학 최신지견 따라잡기
- 진료지침
