이달의 증례
- 페이지 경로
- HOME > 자료실 > 이달의 증례



|
이달의 중재술 / 2017년 12월 Successful Transcatheter Aortic Valve Implantation via Left Subclavian Artery in A 78-Year Old Female With Small Iliofemoral Arteries |
|||||||||||||||||||||
| 저자 | Jumin Won, MD, Min Chul Kim, MD, PhD, Doo Sun Sim, MD, PhD, Young Joon Hong, MD, PhD, Ju Han Kim, MD, PhD, Youngkeun Ahn, MD, PhD, FACC, FSCAI and Myung Ho Jeong MD, PhD, FACC, FAHA, FESC, FSCAI | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 소속 | The Heart Center of Chonnam National University Hospital | ||||||||||||||||||||
|
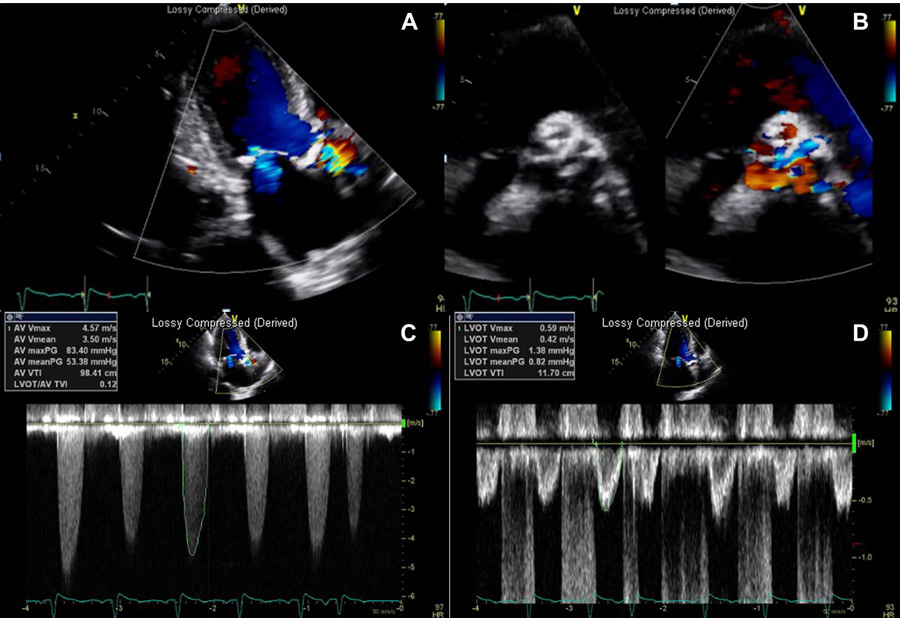
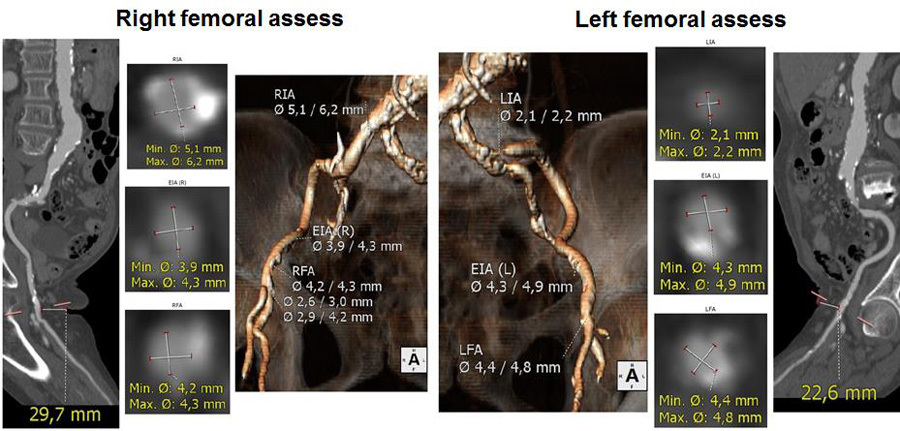
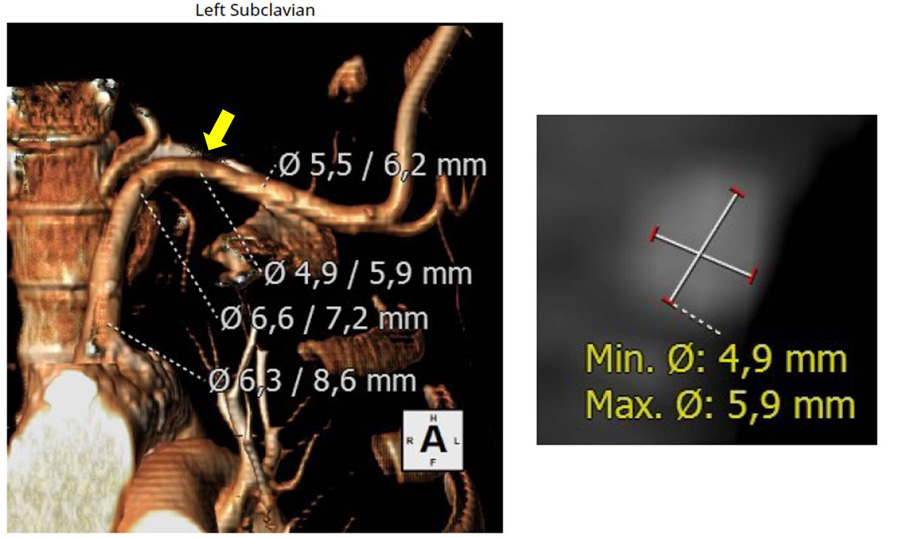
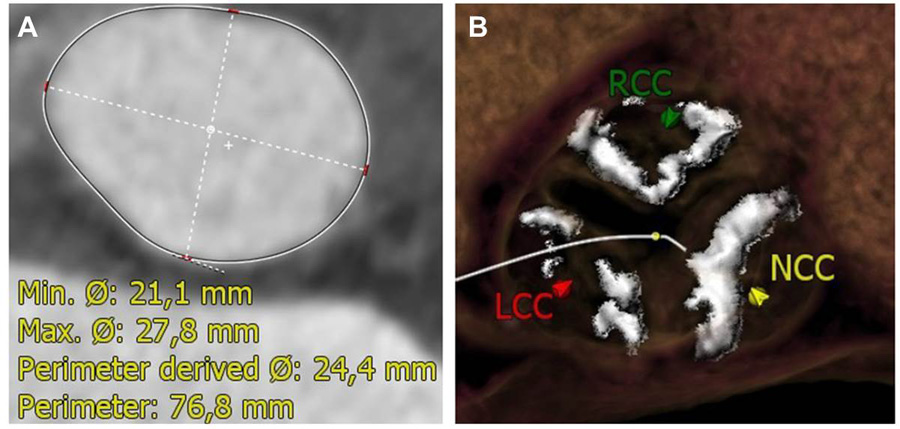
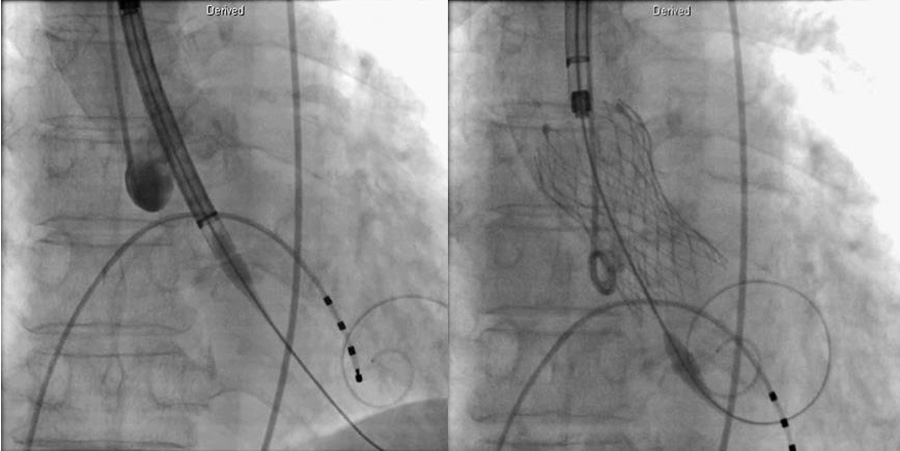
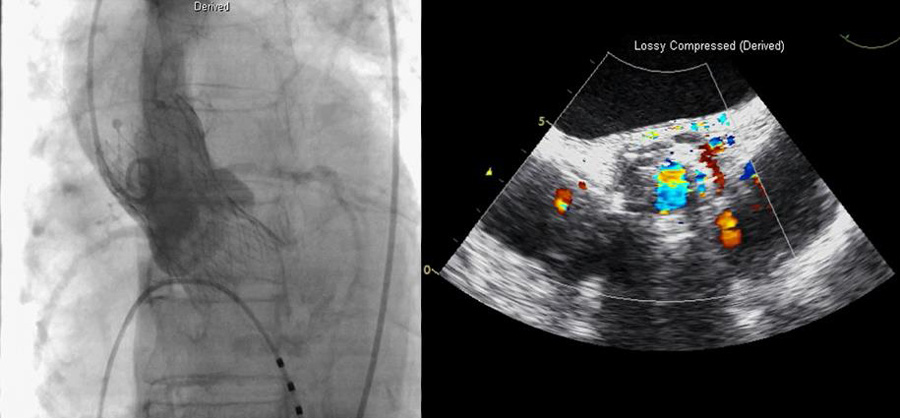
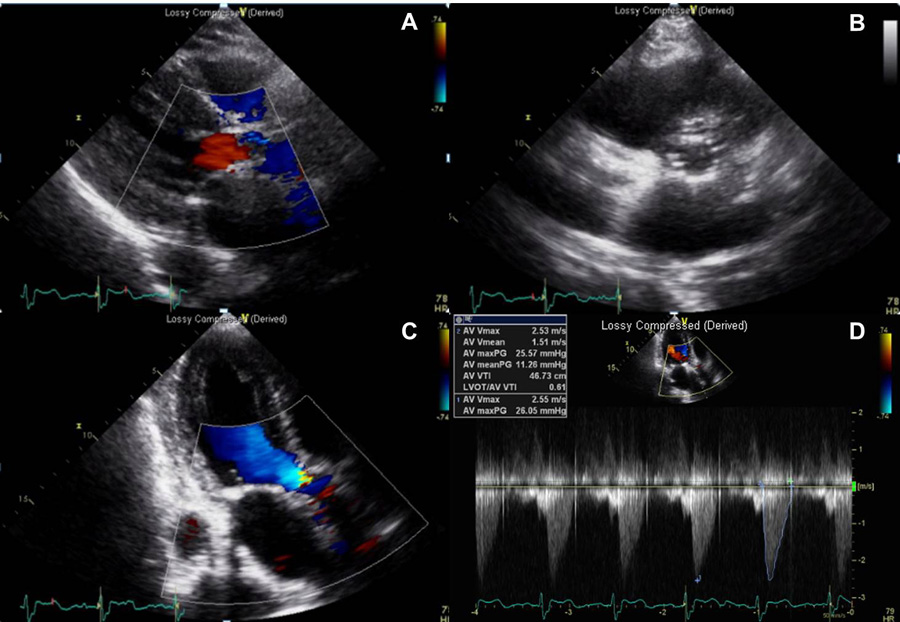
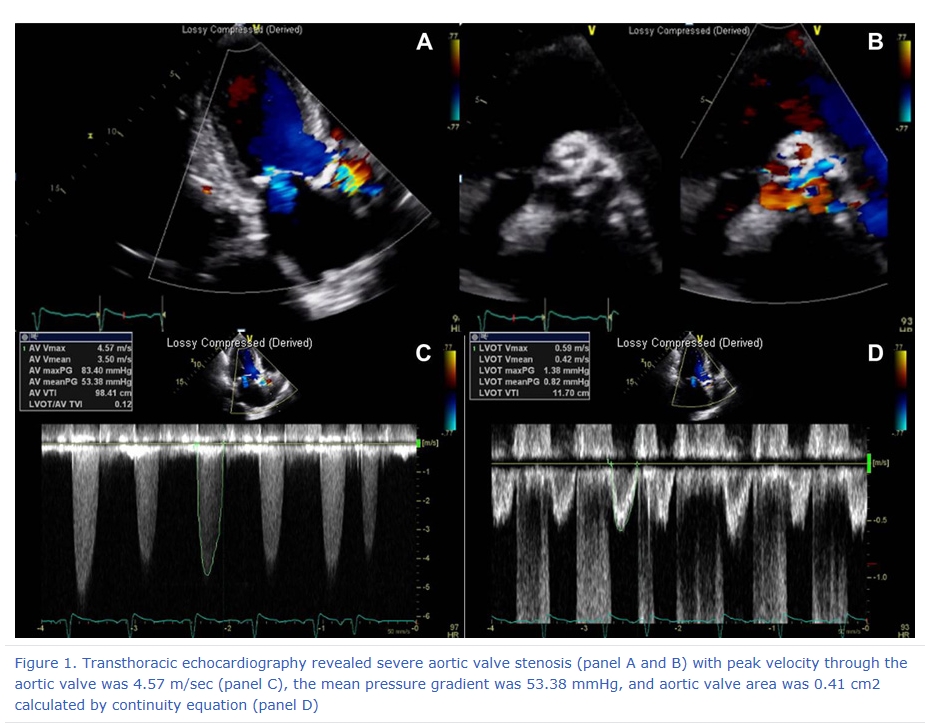
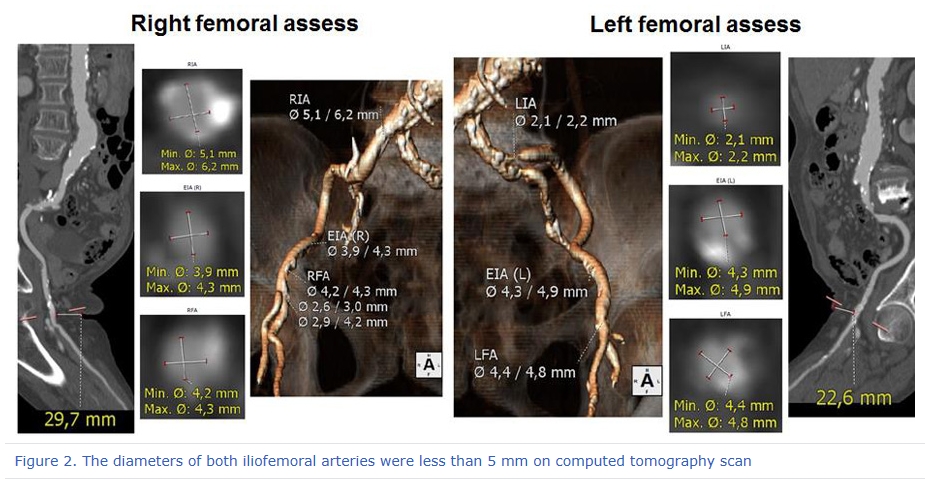
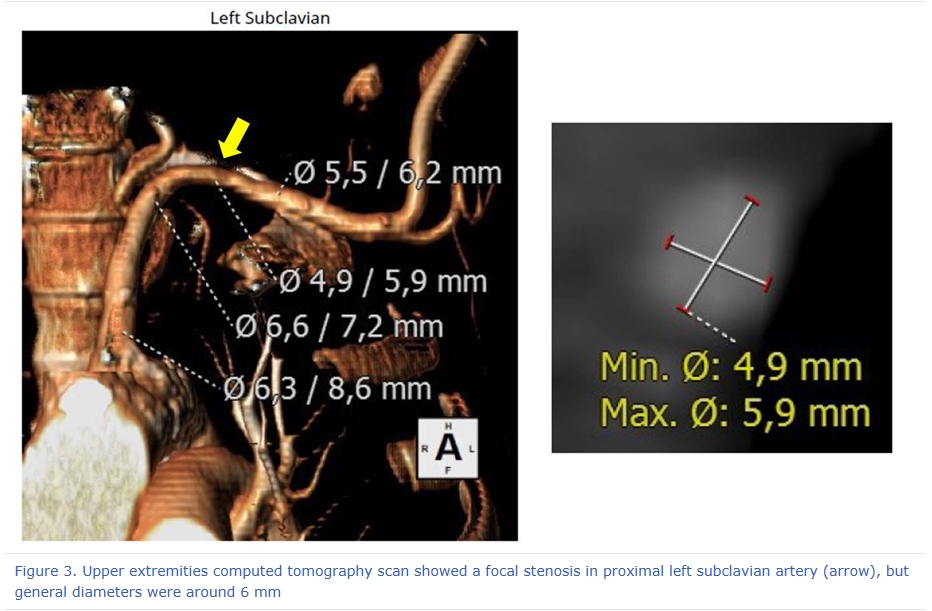
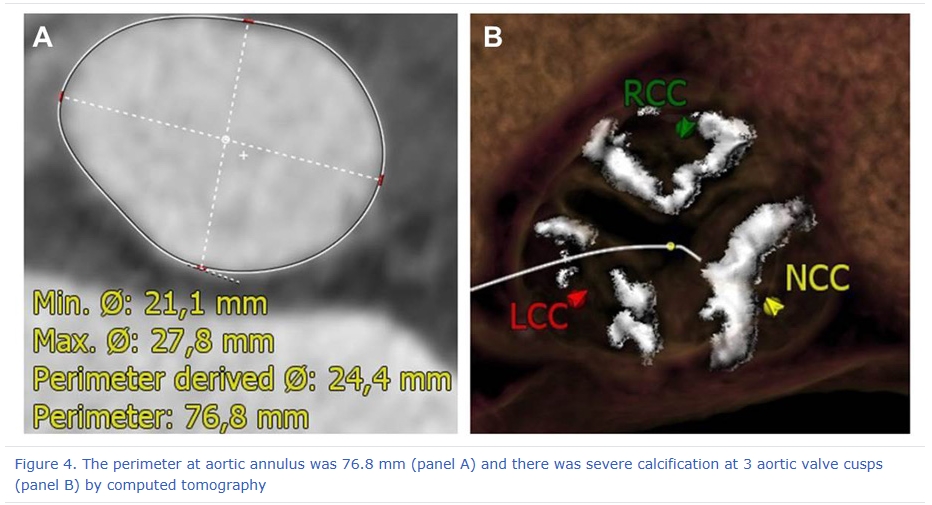
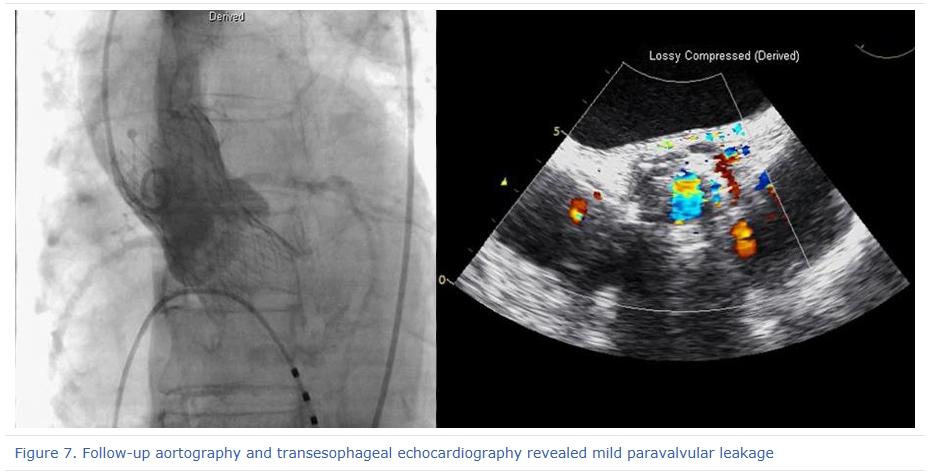
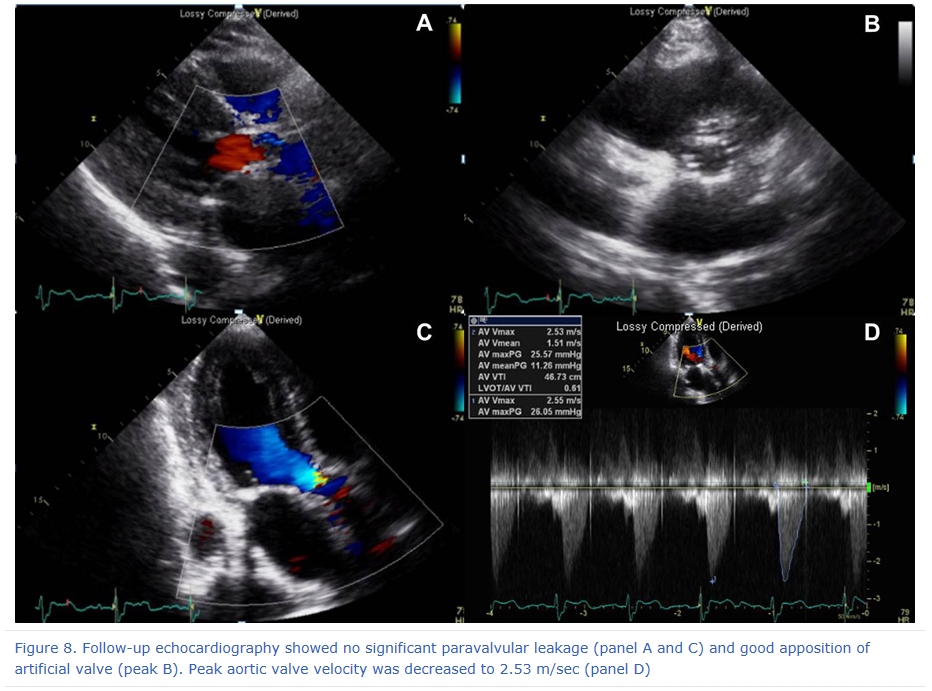
A 78 year-old woman visited Chonnam National University Hospital because of dyspnea and chest tightness which had developed 2 years ago. She had histories of hypertension, and myocardial infarction treated percutaneous coronary intervention for left anterior descending (LAD) artery lesion. On physical exam, systolic ejection murmur was heard on right upper sternal border. Twelve-lead electrocardiogram (ECG) showed normal sinus rhythm, left ventricular hypertrophy, and ST-segment depression on lateral leads which indicated left ventricular hypertrophy strain pattern. Transthoracic echocardiography revealed severe aortic valve stenosis (AS) with peak velocity through the aortic valve was 4.57 m/sec, the mean pressure gradient was 53.38 mmHg, and aortic valve area was 0.41 cm2 calculated by continuity equation (Figure 1). The aortic valve replacement was required, so surgical risk was assessed. The Society of Thoracic Surgeons score (STS) was 8.951% and the European System for Cardiac Operative Risk Evaluation (EuroSCORE) II was 18.54% which indicated high risk for operation. The patient and her protectors did not agree to take a surgical management, so transcatheter aortic valve implantation (TAVI) was planned. Coronary angiography and aortography was performed as pre-evaluations for TAVI. Angiography showed diffuse atherosclerotic lesions, but no in-stent restenosis in proximal LAD stent, or no significant stenosis over both coronary arteries, but tortuous and stenosis with severe calcification over both iliofemoral arteries. The diameters of both iliofemoral arteries were less than 5 mm on computed tomography (CT) scan (Figure 2). To find alternative assess, upper extremities CT scan was checked and it showed a focal stenosis in proximal left subclavian artery, but general diameters were around 6 mm (Figure 3). It could be possible to do TAVI procedure via axillary approach. The perimeter at aortic annulus was 76.8 mm and there was severe calcification at 3 aortic valve cusps (Figure 4). Therefore, 29 mm-diameter self-expandable Evolut R® was selected.
|
|||||||||||||||||||||
| 첨부파일1 | |||||||||||||||||||||
| 첨부파일2 | |||||||||||||||||||||


- Tel 02-3275-5258
- Fax 02-3275-5259
- E-mail herz1@circulation.or.kr
- Copyright© The Korean Society of Cardiology


- 심장학 최신지견 따라잡기
- 진료지침

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}