이달의 증례
- 페이지 경로
- HOME > 자료실 > 이달의 증례



|
이달의 중재술 / 2018년 7월 Successful Percutaneous Coronary Intervention for Simultaneous Culprit Lesions in Patient With ST-Segment Elevation Myocardial Infarction |
|||||||||||||||
| 저자 | Dae Young Hyun, MD, Min Chul Kim, MD, PhD, Doo Sun Sim, MD, PhD, Young Joon Hong, MD, PhD, Ju Han Kim, MD, PhD, Young keun Ahn, MD, PhD, FACC, FSCAI and Myung Ho Jeong MD, PhD, FACC, FAHA, FESC, FSCAI | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 소속 | The Heart Center of Chonnam National University Hospital | ||||||||||||||
|
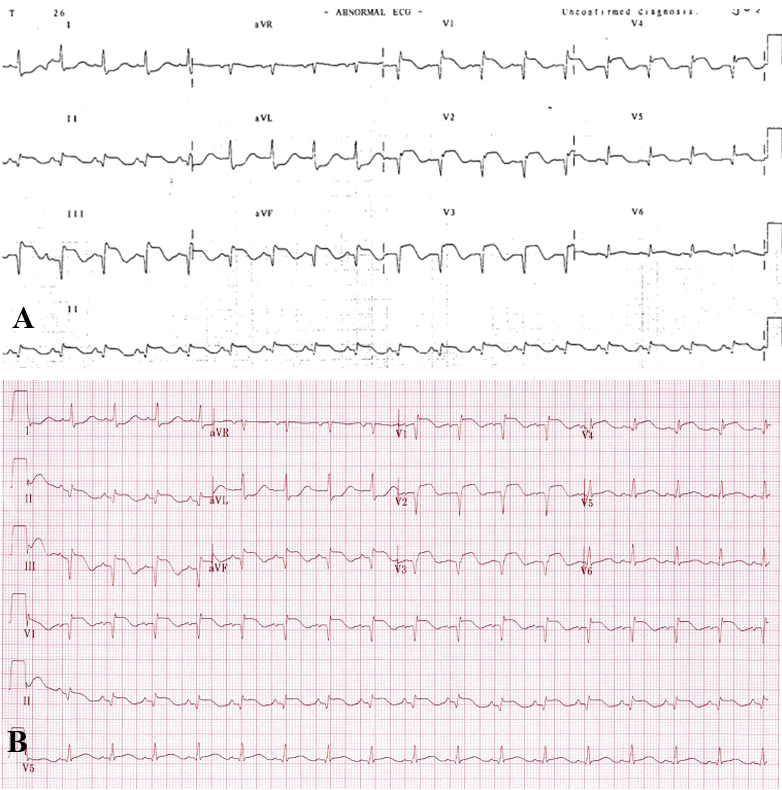
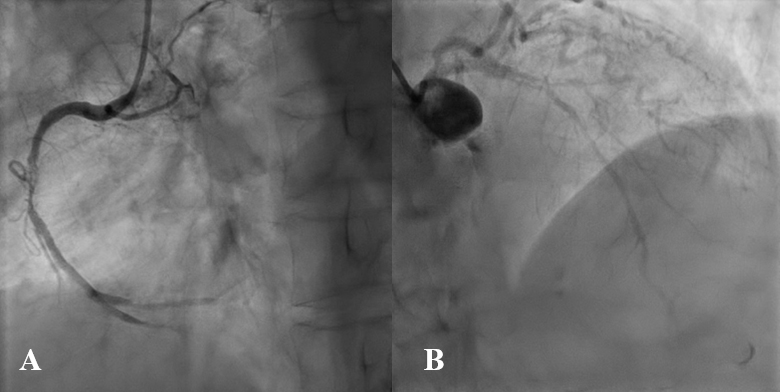
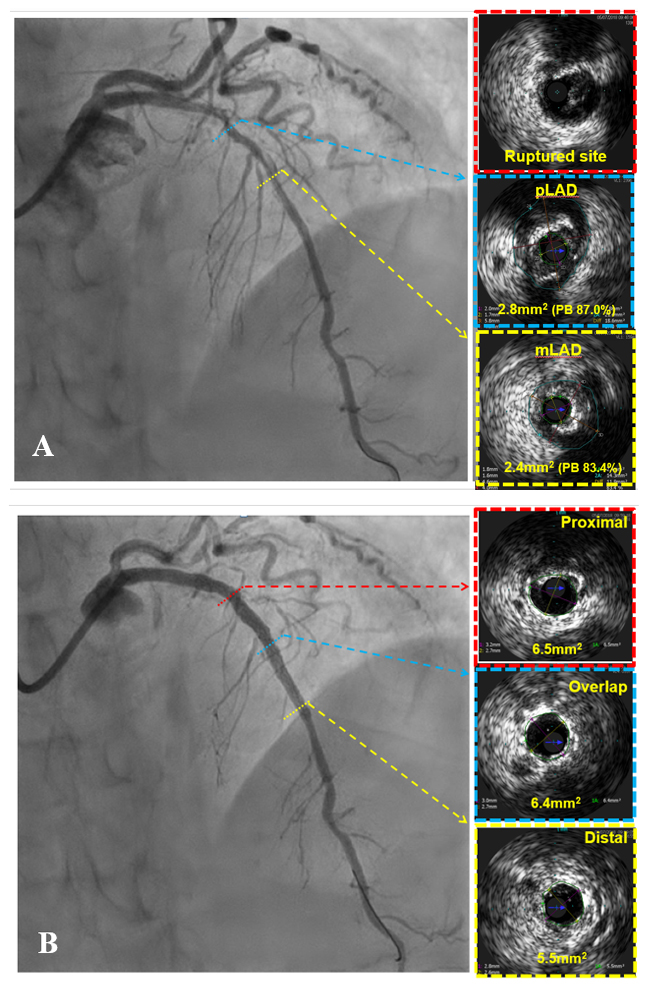
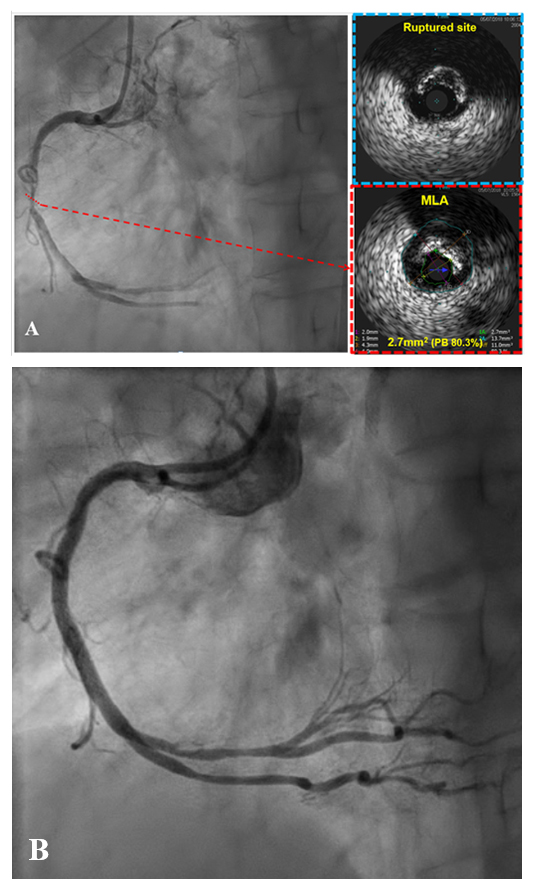
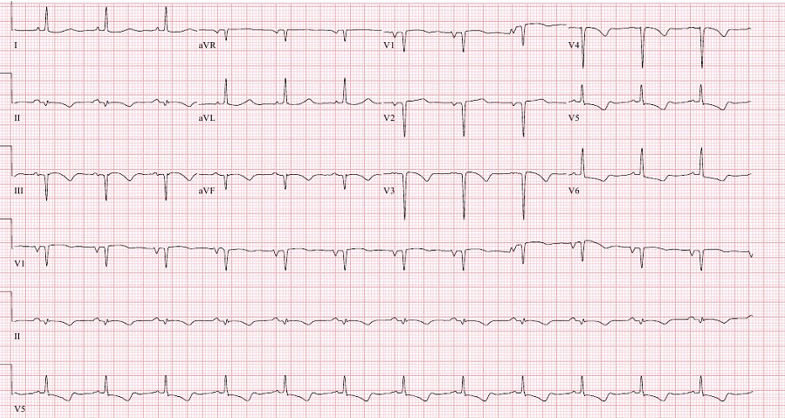
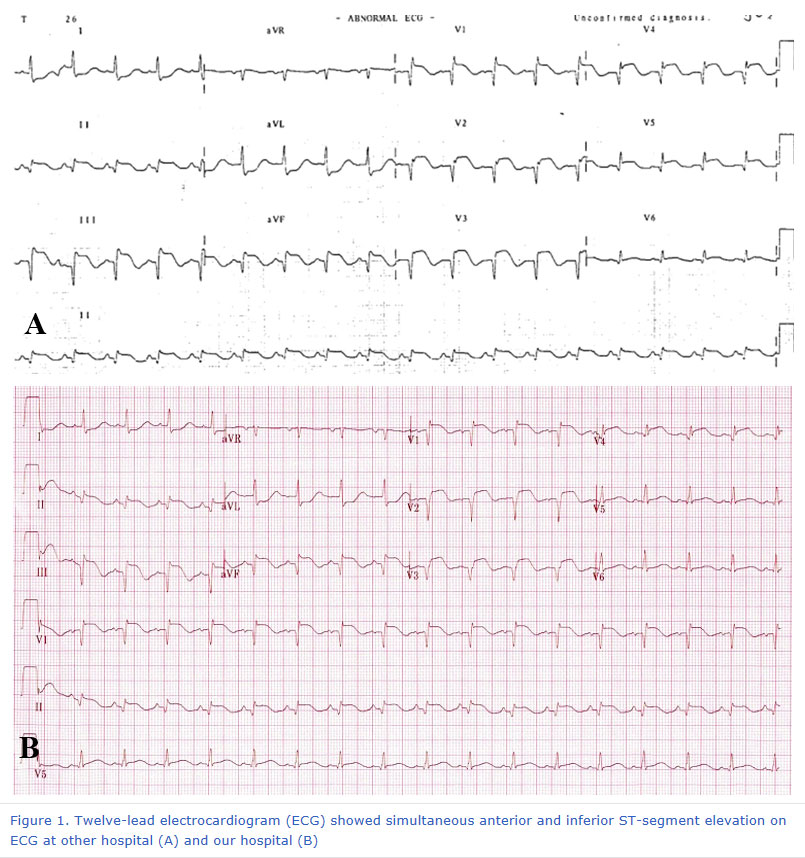
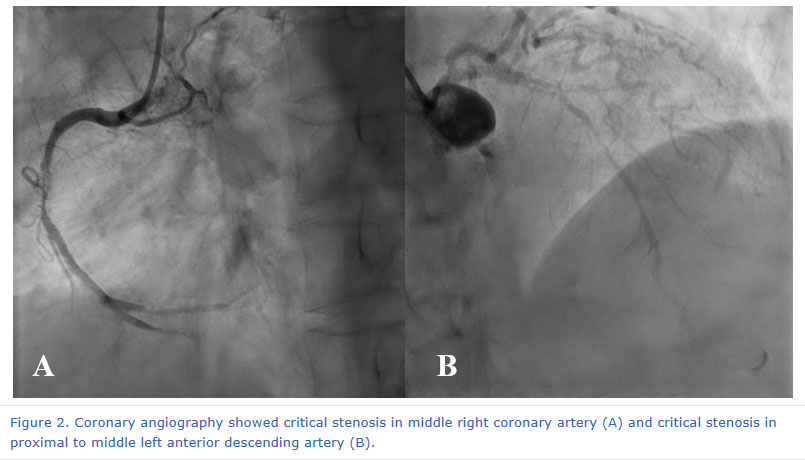
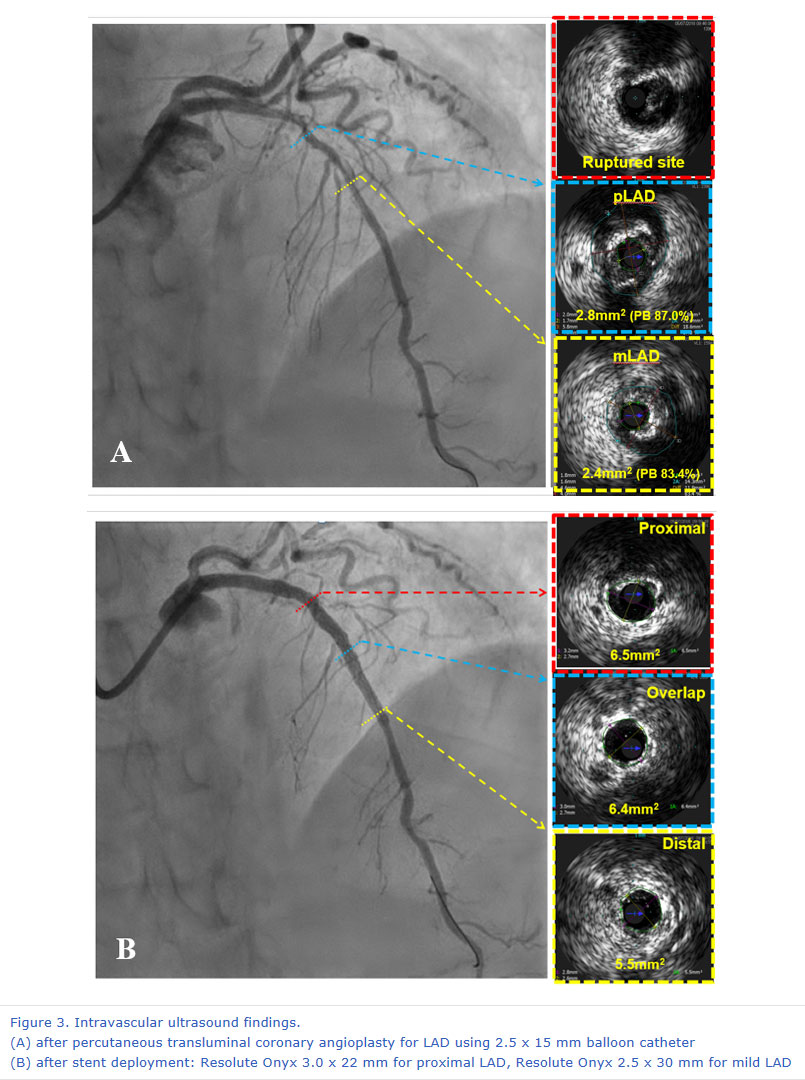
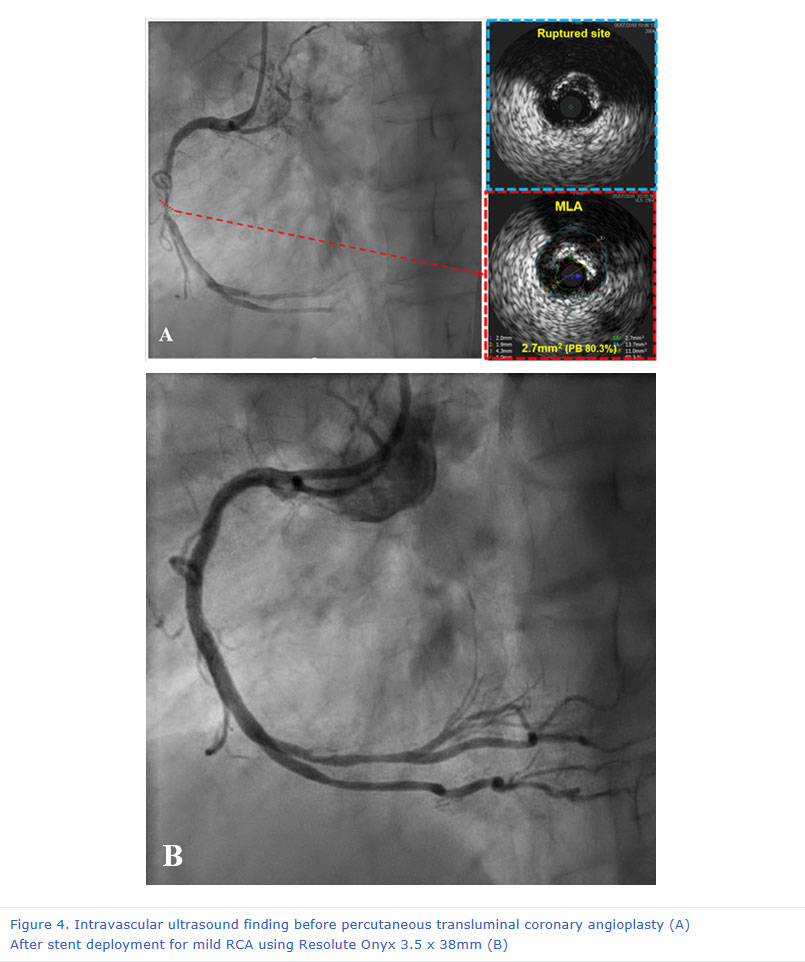
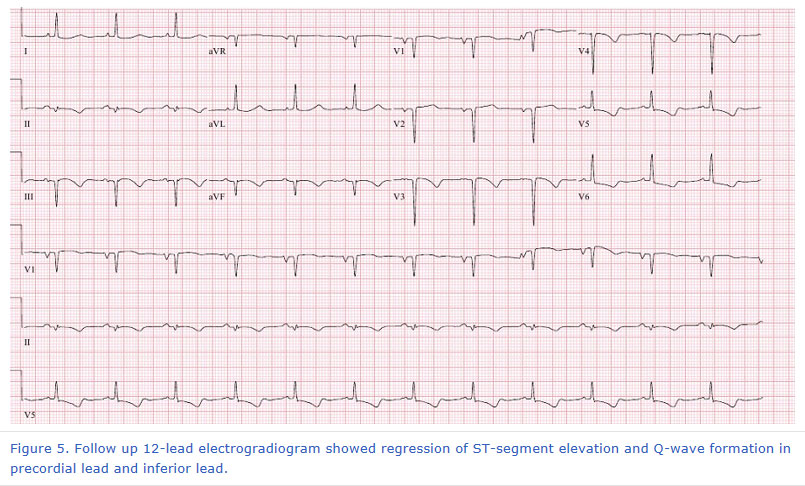
A 74 year old female patient had suffered from chest pain which was developed 6 hours ago. The pain was tearing and not subsided. So she visited nearby hospital. Since there was abnormal finding on 12-lead electrocardiogram (ECG), she was transferred to Chonnam National University Hospital. On 12-lead ECG at other hospital, ST-segment elevation was seen from V1 to V5 and lead II, III, aVF (Figure 1A), and 12-lead ECG at our hospital showed similar finding compared to that achieved at other hospital. (Figure 1B). She had history of cerebral infarction in basal ganglia and cerebellar infarction 1 year ago. Because she complained continuous chest pain and ECG showed simultaneous ST-segment elevation on anterior and inferior leads, we thought that the cause of ST-segment elevation myocardial infarction (STEMI) was vasospasm or thromboembolism. We also considered occlusion of wrapped left anterior descending artery (LAD). Coronary angiography (CAG) revealed critical stenosis in middle right coronary artery (RCA) and critical stenosis in proximal to mid LAD (Figure 2). Firstly, balloon angioplasty was done for proximal to middle LAD using 2.5 x 15 mm balloon catheter, then we examined intravascular ultrasound (IVUS) for LAD. It revealed large amount of plaque burden with plaque rupture in target lesion. Minimal lumen area (MLA) was about 2.4 mm2 and plaque burden was 83% at middle LAD. We implanted 2.5 x 30 mm Resolute Onyx for middle LAD and 3.0 x 22 mm Resolute Onyx for proximal LAD. We also performed additional balloon angioplasty using 3.25 x 12 mm non-compliant balloon for stent under-expansion. Follow-up IVUS showed good stent apposition and expansion, Stent area on proximal was 6.5 mm2 and minimal stent area (MSA) on stent distal part was 5.5 mm2 (Figure 3). Final CAG showed good distal flow without residual stenosis.
|
|||||||||||||||
| 첨부파일1 | |||||||||||||||

- Tel 02-3275-5258
- Fax 02-3275-5259
- E-mail herz1@circulation.or.kr
- Copyright© The Korean Society of Cardiology


- 심장학 최신지견 따라잡기
- 진료지침

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}