Tachycardia-Bradycardia syndrome (TBS) is a variant of sick sinus syndrome in which the arrhythmia alternates between slow and fast heart rates. Usually atrial tachyarrhythmia (atrial fibrillation, atrial flutter or atrial tachycardia) preceded and pause followed sequentially. According to dependence of clinical symptom, permanent pacemaker was considered for bradycardia at first or rhythm control was considered for tachycardia instead of permanent pacemaker implantation.
I would like to introduce two cases of TBS patients whose job are car driver, first case was tachycardia dependent and was treated with rhythm control (atrial fibrillation radiofrequency catheter ablation, AF RFCA) and the other case was tried rhythm control strategy (AF and atrial fibrillation RFCA) but bradycardia with very long pause was sustained just after atrial flutter termination, then permanent pacemaker was implanted five days after RFCA.
Case 1
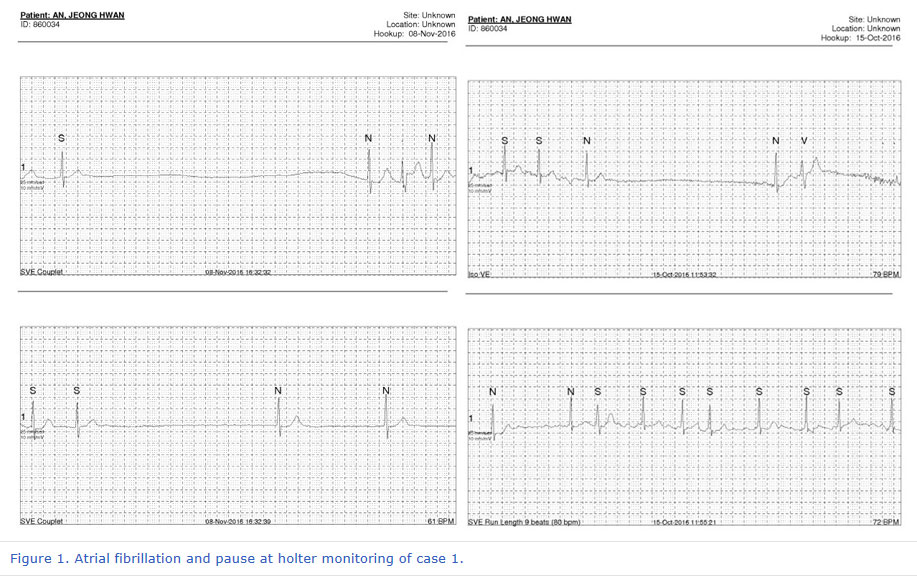
A 54 years old man was visited with syncope. He was truck driver and complained a few seconds of fainting many times during traffic signal waiting just after palpitation. Baseline ECG was sinus but atrial fibrillation (AF) was founded in exercise test. 24 hours holter monitoring showed AF with rapid ventricular response following pause more than 5 seconds (maximal 5.4 sec) many times. He had antiarrhythmic drug but AF with pause was observed continuously at holter monitoring despite of medication. (figure 1)
We planned AF radiofrequency catheter ablation (RFCA) and pulmonary vein isolation (PVI) with cavotricuspid isthmus (CTI) ablation was done sequentially. After the RFCA, no more AF, atrial flutter (AFL) and premature atrial contraction (PAC) were observed during high dose isoproterenol infusion (10 mcg/min) with induction maneuver.
After the procedure, he did not feel palpitation or fainting anymore and 3 months follow up holter monitor showed no AF recurrence. He stopped antiarrhythmic medication and followed at out-patient department (OPD) more than one year.
Case 2
A 65 years old man was visited emergency room (ER) due to syncope with traffic accident. He was taxi driver and felt palpitation and dizziness many times. Baseline ECG was AF and AFL. 24 Hr Holter monitoring showed paroxysmal AF following sinus pause less then 2 seconds. He had antiarrhythmic drug but felt palpitation following dizziness and AF was recurred without definite pause.
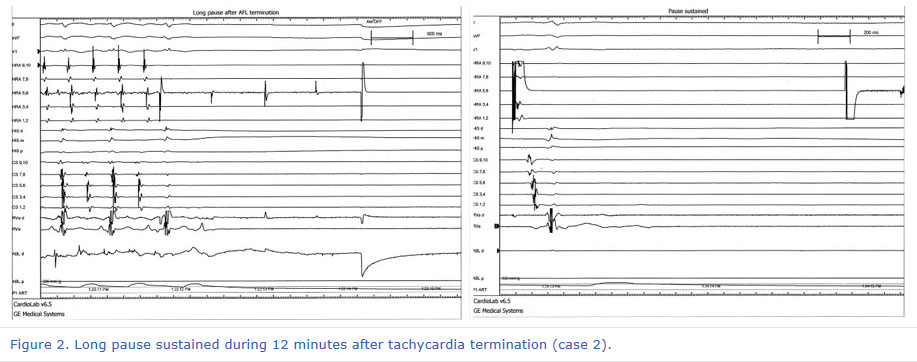
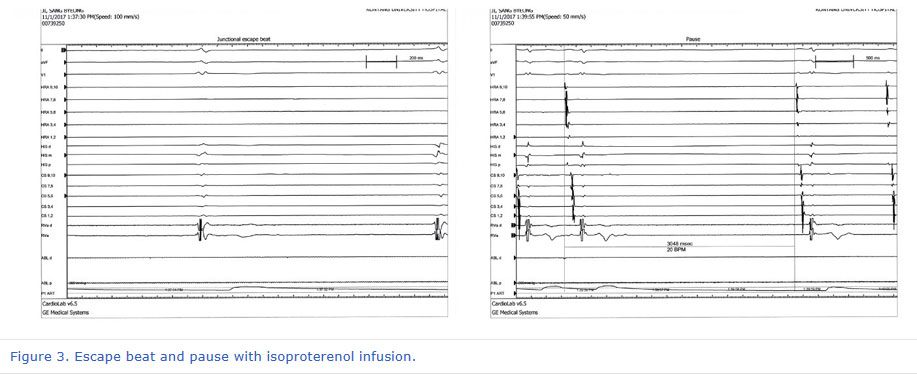
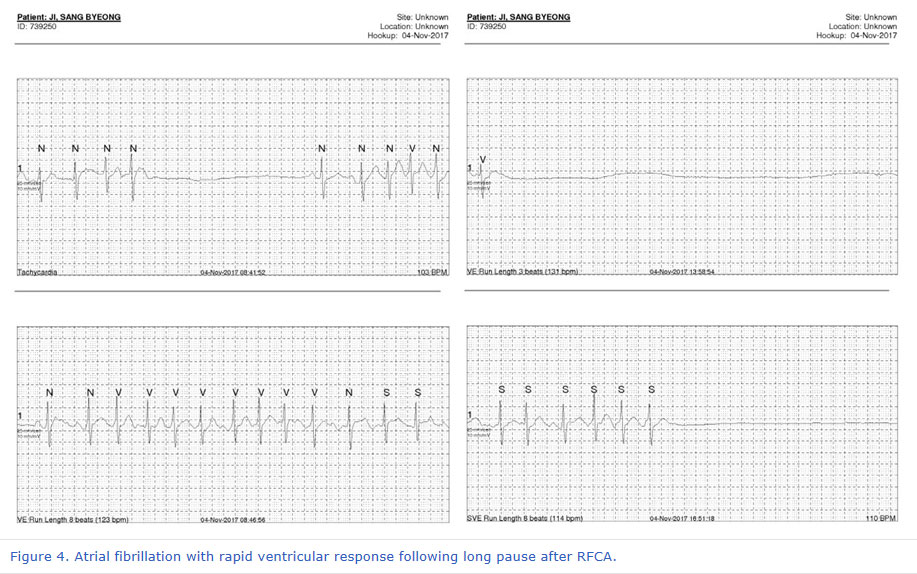
We planned RFCA for drug refractory symptomatic paroxysmal AF and AFL. On electrophysiologic study (EPS), intracardiac electrogram (EGM) showed counter-clockwise AFL, then CTI ablation was performed first. Very long pause was observed just after AFL was terminated and atrial pacing was done. (figure 2) Very rare atrial activity was observed but spontaneous sinus activity did not recovered then isoproterenol infusion was tried. Total pause time was 728 seconds (12 minutes) and recovered to sinus bradycardia with pause keeping isoproterenol infusion (heart rate 30~40 bpm). (figure 3) Further RF ablation was done (PVI) and procedure finished. But bradycardia with escaped beat was frequently observed and patient felt dizziness and as if to faint. Holter monitoring was done three days after RFCA, paroxysmal AF and long pause was observed. (figure 4) Permanent pacemaker was implanted for symptomatic bradycardia and pause. Patient did not feel dizziness anymore and followed up at OPD for two months. 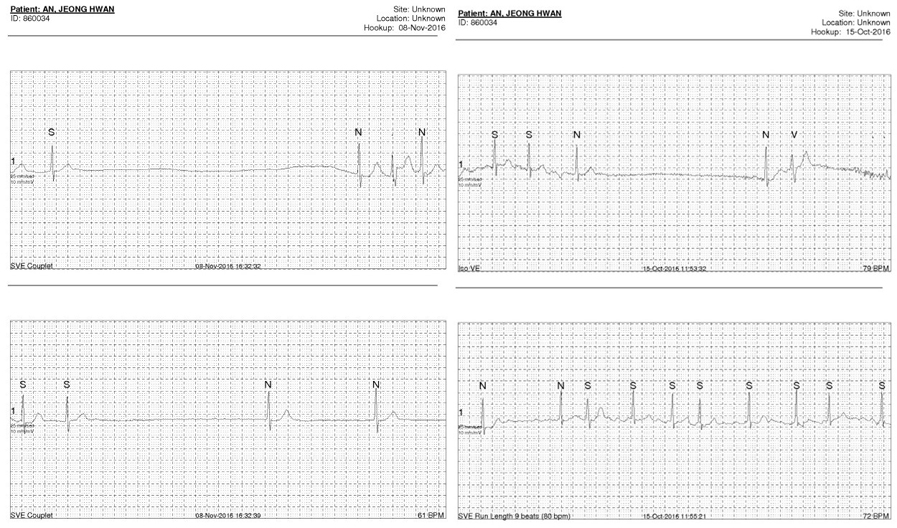 | Figure 1. Atrial fibrillation and pause at holter monitoring of case 1. | 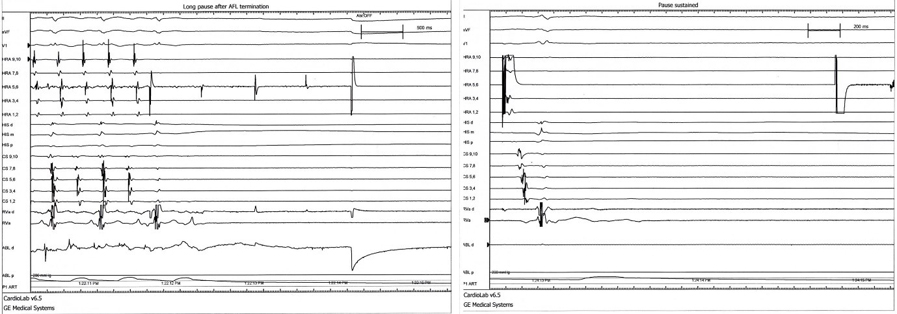 | Figure 2. Long pause sustained during 12 minutes after tachycardia termination (case 2). | 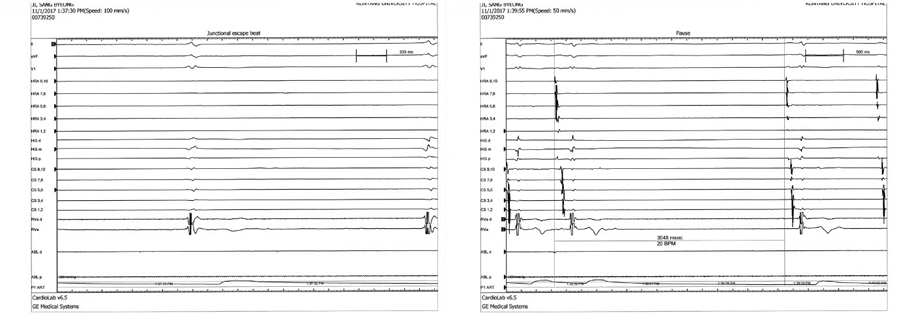 | Figure 3. Escape beat and pause with isoproterenol infusion. | 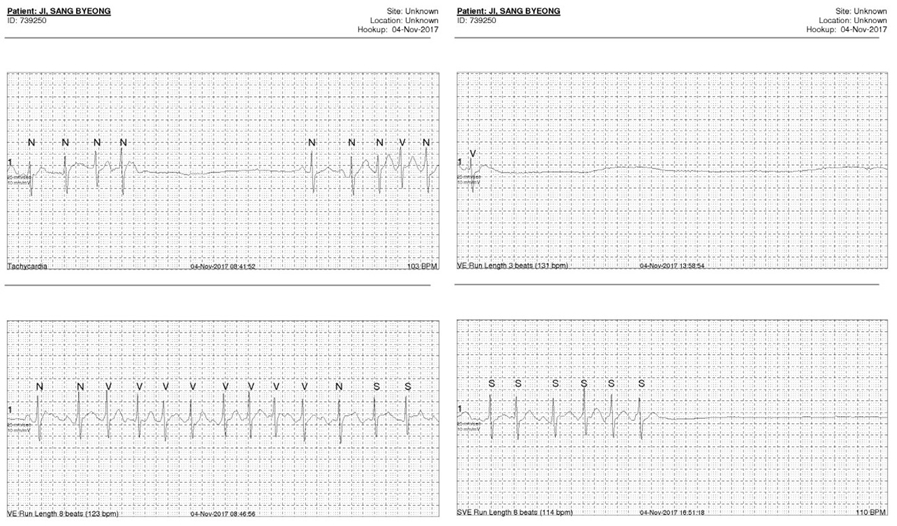 | Figure 4. Atrial fibrillation with rapid ventricular response following long pause after RFCA. |
|







{kind=link}
{kind=link}
{kind=link}
{kind=link}