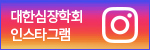
A 54-year-old woman was referred to our emergency department with chest pain and dyspnea lasting to 3 hours. She had a radiating pain to left neck and shoulder. Her vital signs were stable except for sinus tachycardia (111 beats per min). Electrocardiogram showed Q waves and ST-segment elevations in V1, V2 and aVR leads and reciprocal ST-segment depression in II, III, aVF, I, aVL and V5 and V6 leads.(Figure 1) Laboratory tests showed elevations of CK-MB (52.27ng/ml) and Troponin-T (0.421ng/ml). She underwent emergent diagnostic coronary angiography due to suspected acute myocardial infarction of left main coronary artery.
Coronary angiography revealed severe vasospasm with more than 90% stenosis in ostium of the left anterior descending artery. (Figure 2) Also diffuse spastic appearance was revealed in left circumflex artery. Both arteries were subsequently relieved after the administration of sublingual and intracoronary nitrate.
Further investigation revealed an elevated serum free tyroxine of 5.43 ng/dl (normal range: 0.89 to 1.76 ng/dl), suppressed thyroid-stimulating hormone of 0.01uIU/ml (normal range: 0.55 to 4.78 ng/dl), elevated thyroglobulin antibody of 71.7 U/mL (normal value : < 60 U/ml), and elevated TSH receptor antibody of 8.25 IU/L (normal value : < 1.75 IU/L). Goiter with increased trapping in both thyroid lobes in patient's thyroid scan, confirmed the diagnosis of Graves' disease. She was started on methimazole for hyperthyroidism and nifedipine for coronary vasospasm. After that she did not complain chest pain and discharged without apparent sequelae.
The Prevalence of coronary artery spasm with thyrotoxicosis is not high, about 7.4%, and more frequent in females and in younger age groups with few traditional coronary risk factors. In fact, there is no good explanation for this phenomenon. But, some studies have been proposed for the mechanism of thyroid hormone induced coronary vasospasm. During a thyrotoxic state, hypersensitivity to vasoconstrictive agents, decreased vasodilatation, and increased heart rate and increased contractility lead to increased oxygen demand. Therefore, vasospasm by hyperthyroidism should be considered as a cause of acute coronary syndrome. 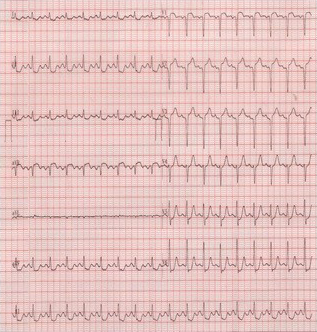 | Figure 1. | 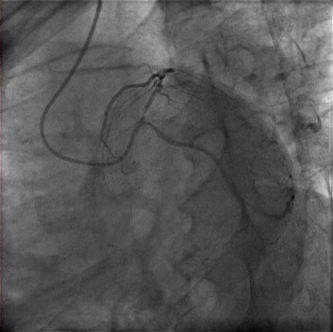 | Figure 2. |
|







{kind=link}
{kind=link}