Introduction: Catheter ablation for atrial flutter (AFL) in patients with large atria is sometimes difficult to achieve isthmus block mostly due to anatomical issues. The purpose of this study is to assess the usefulness of ICE in AFL ablation and cavotricuspid isthmus (CTI) evaluation in patients with large right atrium.
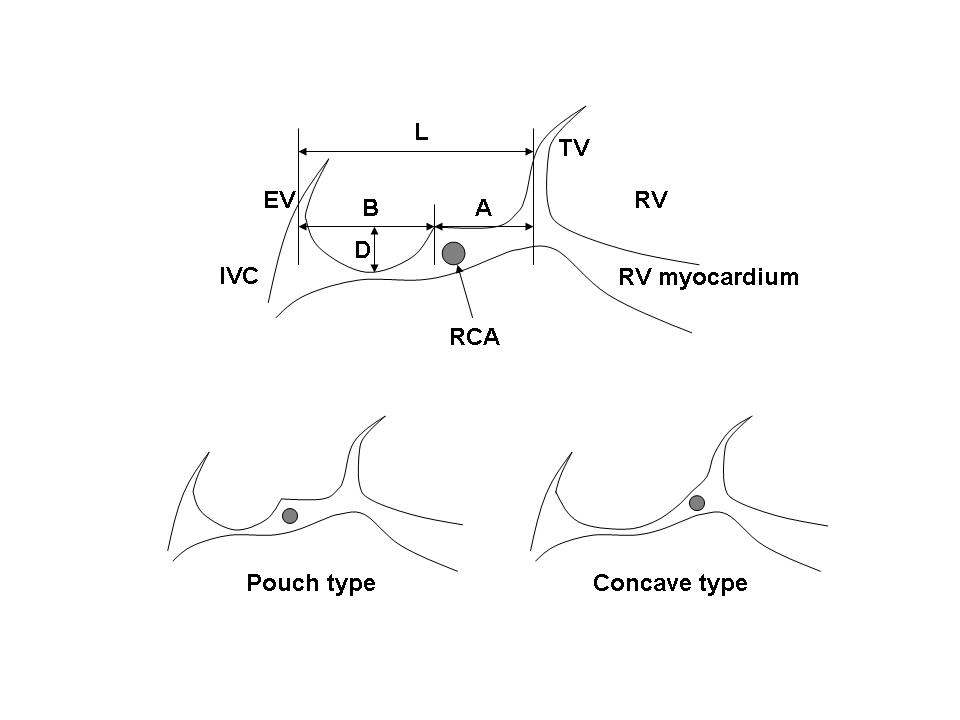
Methods: Patients with typical CTI-dependent AFL and large right atrium (area > 20 cm2 in a 4-chamber view) were enrolled from October, 2006 through June, 2007. If ablation with an 8-mm tip catheter was not successful, the initial ablation catheter was switched to new one with other curve type or a 4-mm tip. ICE was used for all patients. Anatomical dimensions of CTI were measured using ICE system (figure): the lengths of CTI (L) and vestibular area (A), the length (B) and depth (D) of pouch area, and the depth of right coronary artery (RCA).
Results: Total five patients were enrolled in this study. Three patients were pouch type and two were concave type (figure). Each dimension was as follows: L 53ТБ24 mm; A 26ТБ21 mm; B 40ТБ11 mm; D 5ТБ1 mm; RCA depth 4ТБ2 mm. CTI bidirectional block was achieved in four patients.
Conclusion: ICE would be one option for difficult cases in AFL ablation. CTI length of patients with large right atrium was remarkably longer than that of normal population although the depth of pouch area was within normal range.
|