| ьДьэЌТЙ, ъЙььЁАТЙ , ъЙь
ТЙ , ыАьЂ
ь ТЙ , ь ыъЕЌТЙ , эьЙэИТВ , ъЙьЂ
ьЇТГ , ьЁАыЊ
ьАЌтД , ь ыЊ
эИ5, э KAMIR ьАъЕЌь |
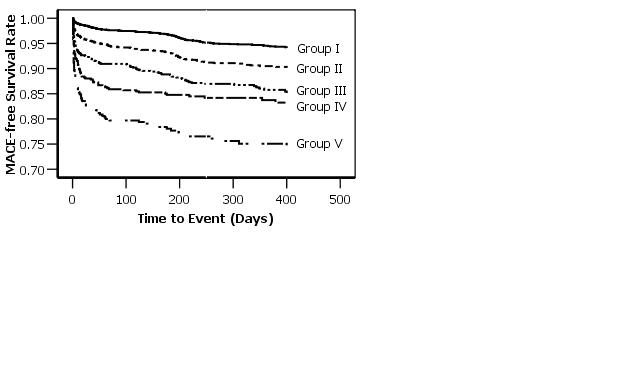
Background: Renal failure is one of the risk factors in prognosis of acute myocardial infarction (AMI). However, the effect of subclinical renal dysfunction on outcomes after AMI is not yet established. Methods: As part of KAMIR study, from December 2005 to February 2007, 6834 patients with serum creatinine between 0.8 and 2.0mg/dl were enrolled. The renal function was defined by estimated glomerular filtration rate (eGFR) using Mayo-eGFR equation and divided into 5 groups as follow; Group I: >90 (n=3441), Group II: 75.0тМ89.9 (n=1649), Group III: 60тМ74.9 (n=881), Group IV: 45тМ59.9 (n=520), Group V: <45 (n=343) ml/min/1.73m2. The major cardiac events (MACE) including death, MI, revascularization rate were compared among groups. Results: Diabetes, hypertension, previous MI, Killip class > I, or left ventricular ejection fraction (LVEF) <40% increased with declining eGFR (p<0.05). On the contrary, reperfusion therapy was more commonly performed in high eGFR groups (p<0.05) in ST-segment elevated MI patients. The prescription rate of aspirin, clopidogrel and beta-blocker was lower in poor eGFR groups (p<0.05). Total MACE were increased with declining eGFR (Figure). Multivariate analysis revealed that the renal function by eGFR (hazard ratio: Group II=1.13, Group V=2.54, p<0.01), LVEF (OR=2.124, p<0.05) were important risk factors for MACE after AMI. Conclusion: Subclinical renal dysfunction, estimated by Mayo-eGFR, should be considered as a strong risk factor for MACE and mortality in AMI patients.
Figure 1. The rate of survival from total events.
|