| мЖ°нШЬкЈЉ ¬є, мЖ°мҐЕлѓЉ ¬є,нЩ©кЄ∞мЫР ¬є,м£ЉмДЭм§С¬≤ ,м†Хм≤†нШД¬≤ ,мЭімЮђмЫР¬≤ ,кєАлМАнЭђ ¬є,к∞ХлНХнШД ¬є,мЖ°мЮђкіА ¬є |
Background: The optimal timing for tricuspid valve (TV) surgery in patients with severe isolated severe tricuspid regurgitation (TR), and clinical outcomes after such operation remain to be established.
Methods: Pre-operative clinical and echocardiographic characteristics were evaluated in 50 consecutive patients without significant left-sided valvular heart disease who underwent single TV surgery (TV repair in 40, TV replacement in 10). Etiology of TR was functional in 40 patients. Atrial fibrillation was shown in 28, and Maze operation was performed in 11. All-cause mortality was followed-up for median of 43.5 months.
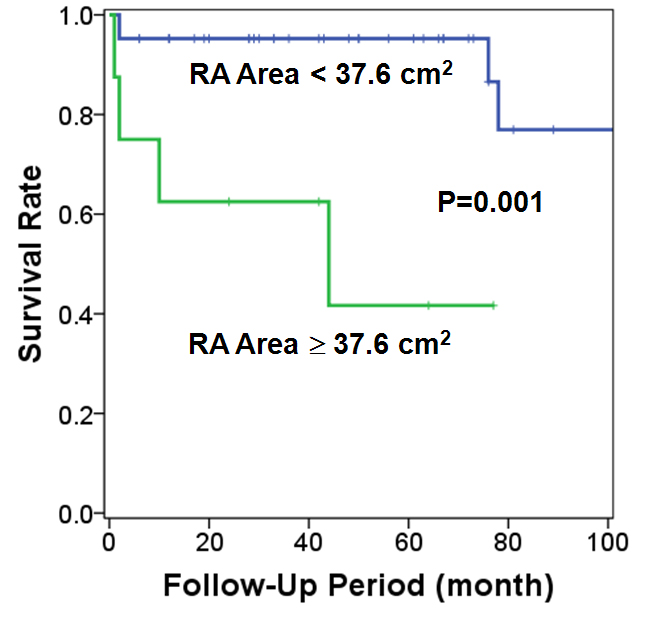
Results: Of 50 patients, 4 (8%) and 4 (8%) died after TV surgery before discharge, and during follow-up period after discharge, respectively. The 8 patients who died had a larger pre-operative right atrial (RA) area measured from apical 4-chamber view (44.9±26.7 vs. 30.9±7.4 cm2, p=0.005), and a larger right ventricular (RV) diastolic dimension measured from parasternal long-axis view (45.7±13.0 vs. 38.9±7.2 mm, p=0.04) than 42 patients who survived. Hemoglobin level tended to be lower in the former than the latter group (11.9±3.3 vs. 13.2±2.0 g/dL, p=0.14). Pre-operative atrial fibrillation, pulmonary artery pressure, TR severity, and RV areas and fractional area change were not significantly different between the 2 groups. By multivariate Cox proportional hazard model, a pre-operative large RA area (hazard ratio: 1.034 per 1 cm2, 95% confidence interval: 1.007-1.061, p=0.012) was the only major predictor for mortality. RA area of 37.6 cm2 was the best cutoff value by ROC curve analysis. The 8 patients with pre-operative RA area 37.6 cm2 showed lower 5 year survival rate than 42 patients with RA area < 37.6 cm2 (42±21% vs. 95±3%, p=0.001, Figure).
Conclusion: Pre-operative RA area is the best predictor for mortality after single TV surgery, thus surgery should be considered before RA significantly dilates in patients with severe isolated TR.
|