Backgroud: Prolongations of PR interval and QRS duration in 12-lead ECG are associated with atrioventricular and inter/intraventricular dyssynchrony, respectively. However, their clinical significance remains unclear in patients presenting with acute heart failure.
Methods: We assessed whether presence of PRвЙ•200msec. and/or QRSвЙ•120msec. was associated with poor clinical outcomes in 1985 patients with acute heart failure in sinus rhythm registered in KorHF registry. They were divided into three groups depending on the presence of none, either, or both prolonged intervals; score 0, 1, and 2 groups, respectively.
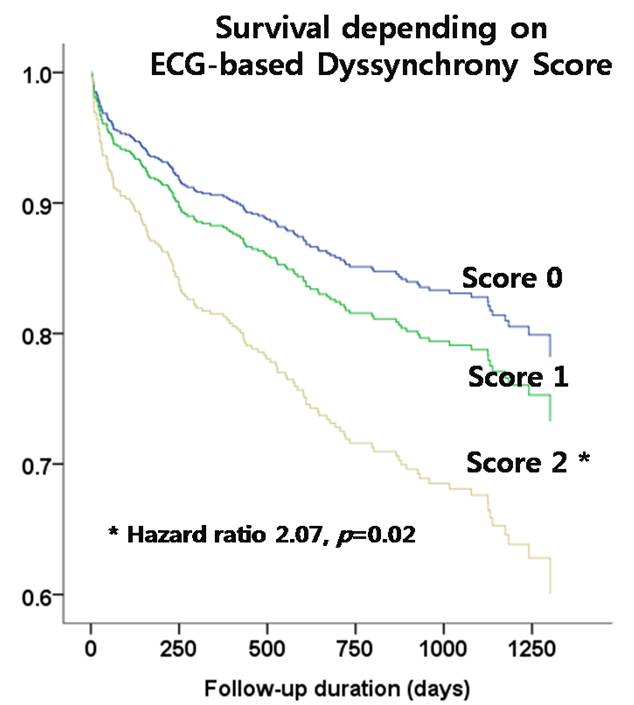
Results: Left ventricular ejection fraction decreased significantly as the score increased (39¬±15%, 38¬±16%, and 34¬±15%, p<0.01) and there was a trend toward longer duration of hospital stay (13¬±16, 13¬±16, and 16¬±35days, p=0.19) in patients with larger score. Re-admission rate within 1 year was significantly higher in patients with score 2 (17.0% vs. 24.2% vs. 29.3%; p=0.03). During a mean follow-up of 19¬±14 months, incidences of mortality significantly increased depending on the score (17.1% vs. 20.4% vs. 29.0 %; p<0.01 for trend). Presence of both PRвЙ•200msec. and QRSвЙ•120msec was identified as an independent predictor of long-term mortality after adjusted for age, sex, heart rate, ejection fraction, presence of ischemic heart disease, and beta-blocker use (Hazard ratio, 2.07; 95% confidence interval, 1.12 to 3.86; p=0.02).
Conclusion: A combined analysis using ECG-based dyssynchrony markers (prolonged PR interval and QRS widening) might be useful for short and long-term risk stratifications of patients presenting with acute heart failure.
|