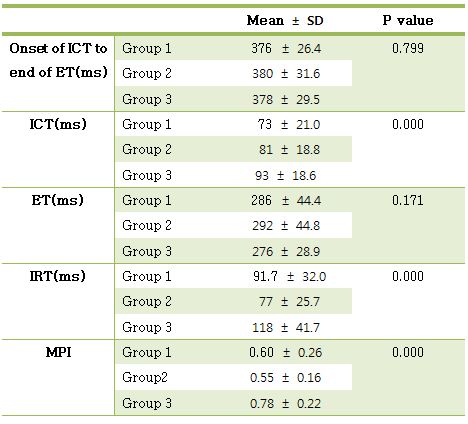
Introduction: Papillary muscle, one of mitral apparatus, is vital to maintaining mitral valve competence. During isovolumic relaxation time, negative pressure arise from relaxation of ventricular myocardium in LV and positive pressure arise from pulmonary venous return in LA. Nevertheless, no blood flow occur from LA into LV during isovolumic relaxation time before opening of mitral valve. We hypothesize that papillary muscles would contract more longer and relax more later than other portion of LV to prevent mitral valve opening. Methods: Forty patients without significant cardiac abnormalities on echocardiograms were studied. Tissue Doppler imaging was obtained with the sample volume placed at the mitral medial annulus(group 1), lateral annulus(group 2) and posteromedial papillary muscle(group 3) from the apical 3 or 4-chamber view. The isovolumic contraction time(ICT) and isovolumic relaxation time(IRT) were measured from the end of the mitral annular velocity pattern to the onset of the S-wave and from the end of the S-wave to the onset of the mitral annular velocity pattern. The ejection time(ET) was defined the duration of the S-wave. Myocardial performance index(MPI) were calculated as (ICT+IRT)/ET. Result: There were significant differences with ICT, IRT and MPI between group 1, group 2 and group 3(p <0.05)(image 1). But, ICT, ET, IRT and MPI were similar in group 1 and group 2. ICT, IRT and MPI was longer in group 3 than the time in group 1 and 2(p < 0.05). Period from onset of ICT to end of ET which consisted of systolic phase were no significant differences between group 1, 2 and 3. Conclusion: Papillary muscles relax more later and contract more longer than other portion of left ventricle in early diastole. This is perhaps the reason ventricular filling does not occur during IRT. Through papillary muscle contract more longer than LV, papillary muscle maintain mitral valve competence. Keywords: papillary muscle, mitral valve competence, tissue Doppler, isovolumic relaxation time.
|