Background: Antithrombotic recommendations for relatively low risk patients with atrial fibrillation (AF) are not well established. Some patients with CHADS2 score=0 have a CHA2DS2-VASc score of 2, which indicated warfarin therapy in the latter system. We evaluated the thromboembolic risk in AF patients with a CHADS2 score of 0 or 1.
Methods: A total of 695 patients with AF that were followed for вЙ• 12 months (median 65.6 months, range 12-138 months), were analyzed retrospectively. The modified CHADS2 score (MCS) was applied as follows. Each CHADS2 score group was divided into two groups, A and B (i.e. MCS 0A vs. 0B, and MCS 1A vs. 1B) according to the number of non-major risk factors (female gender, chronic kidney disease, coronary artery disease, age 65 to 74 years). Group A had 0 or 1, and group B had 2 or more non-major risk factors.
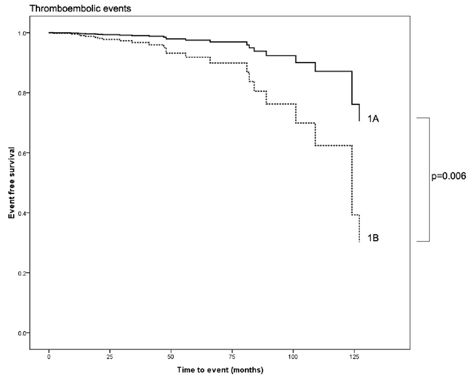
Results: In patients with CHADS2 score=1, there were 13 thromboembolic events (0.65%/year) in 343 MCS 1A patients, and 12 thromboembolic events (1.90%/year) in 108 MCS 1B patients. Thromboembolic risk was significantly higher in the MCS 1B compared to the MCS 1A patients (p=0.006). In 244 patients with CHADS2 score=0, the thromboembolic risk of MCS 0B was similar to that of MCS 0A (p=0.095), and 26 patients had a CHA2DS2-VASc score of 2.
Conclusion: Patients with MCS 1B had a higher thromboembolic risk than patients with MCS 1A. Antithrombotic strategies for patients with a CHA2DS2-VASc score of 2 but a CHADS2 score of 0 need further investigation.
|