Introduction
The simple risk stratification that identify high-risk subsets of patients with unprotected left main coronary artery (ULMCA) stenosis undergoing revascularization has not been well established.
Hypothesis
We assessed the hypothesis that initial clinical indication for revascularization such as stable angina, unstable angina and non-ST elevation myocardial infarction (NSTEMI) may determine the cardiovascular outcomes in patients with ULMCA stenosis.
Methods
Between January 2000 and June 2006, 2,240 patients who underwent stenting (n=1,102) or coronary artery bypass surgery (n=1,138) for the ULMCA stenosis were followed up to at least 3 years and stratified by their clinical indication for revascularization. The end points of the study were the composite of death, Q-wave myocardial infarction, or stroke.
Results
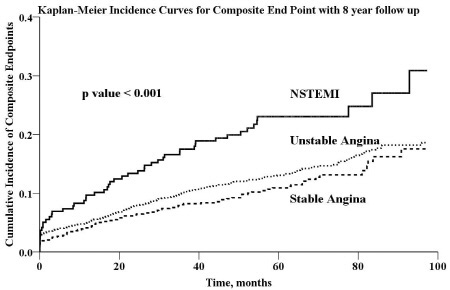
During follow-up period, a total of 352 patients experienced at least 1 event, including 328 with cardiovascular death. Patients with NSTEMI (n=220) had the highest rate of subsequent cardiovascular events (24.8%; 95% confidence interval [CI] 21.5%-28.1%); patients with unstable angina (n=1384) had a lower risk (18.2%; 95% CI 16.9%-19.5); and patients with stable angina (n=636) had the lowest risk (16.1%; 95% CI 14%-18.2%) (P<0.001 for NSTEMI versus stable and unstable angina). In addition, in multivariate analysis, the presence of chronic renal disease (hazard ratio [HR], 4.16; 95% CI, 2.84-6.1; p<0.001), and atrial fibrillation (HR 3.0; 95% CI 1.88-4.77; p<0.001) each were associated with a significantly higher risk of the cardiovascular outcomes.
Conclusions
In conclusion, clinical descriptor such as initial clinical indication for revascularization may assist the clinician in identifying high-risk patients after revascularization for ULMCA stenosis.
|