Background :
Elevated blood homocystein has been suggested as the risk factors for cardiovascular events in several observational epidemiological studies. Little is known regarding the impact of homocystein on clinical outcome after percutaneous coronary intervention (PCI).
Methods :
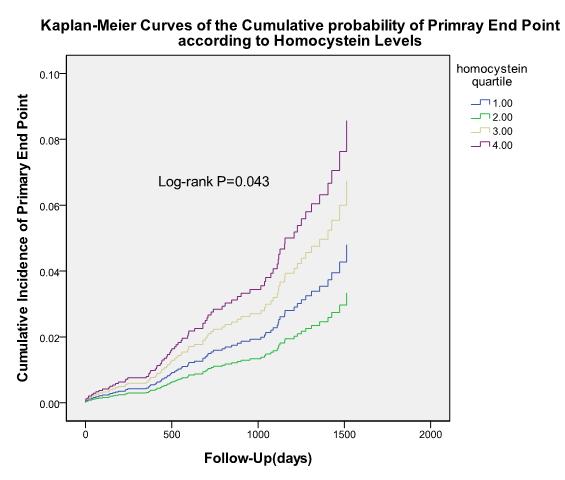
A total of 2,849 patients who received PCI with drug-eluting stent (DES) implantation were prospectively enrolled. Patients were classified 4 groups as quartile of baseline homocystein level (group 1; <10.1umol/L, group2; 10.2 to 12.6umol/L, group 3; 12.7 to 15.1umol/L, group 4; >15.2umol/L). The primary end point was the first occurrence of major cardiovascular events (MACE) defined as a composite of all-cause death, nonfatal myocardial infarction, stent thrombosis, and stroke.
Results :
During follow-up (median, 2.2 years), there were 96 major cardiovascular events. In a crude analysis, patients with the highest quartile of homocystein level was significantly higher risk for the occurrence of the primary end points, as compared to lowest Homocystein level (6.4% vs. 1.0% at 2 year; hazard ration [HR] 1.99, 95% confidence interval [CI],1.17-3.41; P=0.005). After adjusting conventional clinical risk factors and procedural characteristics, increasing levels of serum homocystein was independently associated with higher risk of long-term MACE (adjusted HR 1.79, 95% CI 1.01–3.27., p=0.04).
Conclusion :
Our data suggest that in patient receiving PCI with DES implantation, higher homocystein levels was significantly associated with cardiovascular events and also had incremental predictive values beyond conventional risk factors.
|