| кµђл≥ЄкґМ¬є , лПДм§АнШХ¬≤, Anrejs Erglis¬≥, David DanielsвБі, James Min5, мЦСнХЬл™®¬є, л∞Хк≤љмЪ∞¬є, к∞ХнШДмЮђ¬є, кєАнЪ®мИШ¬є |
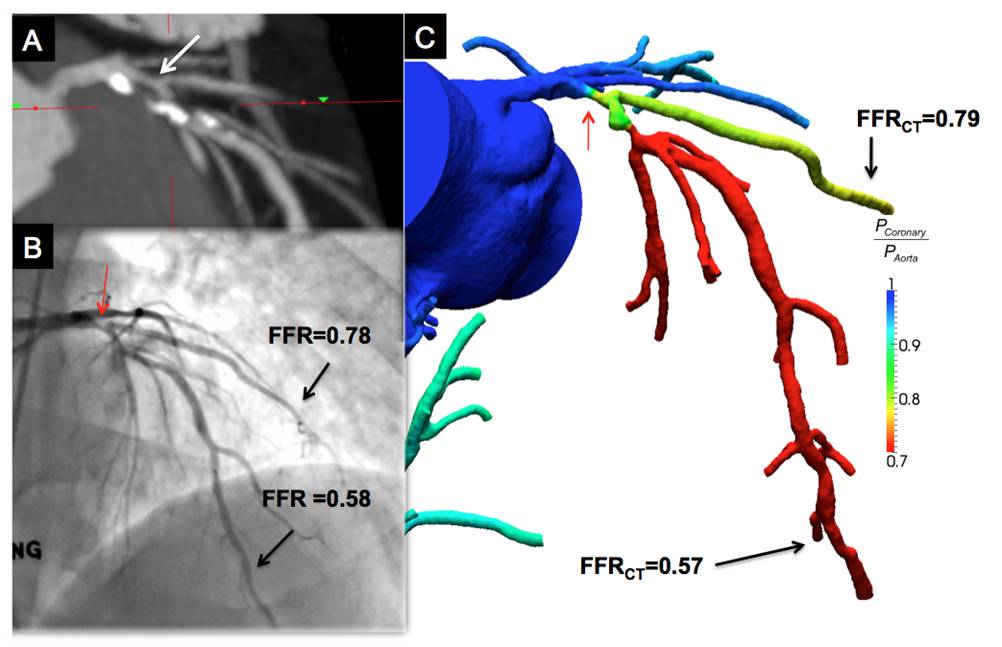
Background: Fractional flow reserve (FFR) is the gold standard for identifying ischemia-causing coronary artery stenosis and improves clinical decision-making for revascularization in patients coronary artery disease. Computational fluid dynamics applied to coronary CT angiograms (CCTA) permits non-invasive calculation of FFR (FFRCT) (Figure), but the diagnostic performance of FFRCT as compared to invasive measured FFR is unknown.
Methods: We conducted a prospective multicenter study to determine the diagnostic performance of FFRCT on 159 vessels in 103 patients. Independent core laboratories determined FFRCT and stenosis severity by CCTA. Ischemia was defined by an FFRCT and FFRвЙ§0.80, and anatomically obstructive stenosis was defined with stenosis вЙ•50%. Diagnostic performance of lesion-specific ischemia was determined for FFRCT and CCTA stenosis relative to an invasive FFR reference standard.
Results: 56% of patients had вЙ•1 vessel with FFRвЙ§0.80. On a per-vessel basis, for the diagnosis of lesion-specific ischemia, accuracy, sensitivity, specificity, positive and negative predictive values for FFRCT were 84.3%, 87.9%, 82.2%, 73.9%, 92.2%, respectively; and for CCTA stenosis were 58.5%, 91.4%, 39.6%, 46.5%, 88.9%, respectively. The area under the receiver operator characteristics curve was 0.90 for FFRCT and 0.75 for CCTA stenosis (p=0.001), with no added discriminatory value of CCTA stenosis to FFRCT (p=0.50). FFRCT and FFR were well correlated (r=0.717, p<0.001) with a slight underestimation by FFRCT (0.022¬±0.116, p=0.016). Similar relationships were observed for diagnostic performance and discrimination for per-patient analyses.
Conclusions: Non-invasive FFR computed from CCTA images is a novel method with high diagnostic performance for the detection and exclusion of coronary lesions that cause ischemia
|