Background Although surgical intervention for patients with subarterial ventricular septal defect (sVSD) to prevent progression of aortic regurgitation (AR) has been recommended, longitudinal follow-up data in adult patients are not available.
Methods Outcome data of 60 adult patients with sVSD (36±13 years) without initial open heart surgery (OHS) were compared with those of age-matched 120 patients with perimembranous VSD (pmVSD).
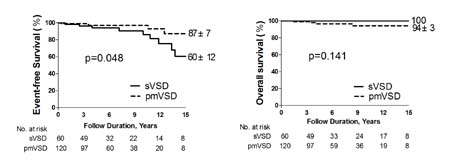
Results Prolapse of aortic sinus wall was more frequently observed in sVSD group (38.3% [23/60] versus 2.5% [3/120], p<0.0001), whereas remnant defect size (3.5±0.9 vs. 3.6±1.3 mm), left ventricular diastolic dimension (52±6 vs. 51±6 mm) and Qp/Qs (1.4±0.2 vs. 1.3±0.2) were not different between groups. During follow-up (90.9±63.4 months), 9 patients underwent OHS due to sinus of Valsalva aneurysm rupture (SVAR, n=4), infective endocarditis (IE, n=3) and heart failure (n=2) in sVSD group, whereas 2 patients needed OHS due to IE and heart failure in pmVSD group. Although 15-year event (OHS, IE and cardiac death)-free survival rate was marginally lower in sVSD group (60±12 versus 87±7%, p=0.048), 15-year over-all survival rate was not different (100 versus 94±3 %, p=0.141). In sVSD group, moderate and severe AR was diagnosed in 3 and 1 patients at initial diagnosis and, except I patient with severe AR, no one needed OHS due to AR progression during follow-up. Development of SVAR was critically dependent on maximal length of prolapsing aortic sinus wall at initial diagnosis and the optimal cutoff value was 7.0 mm with sensitivity and specificity of 100 and 95%, respectively. SVAR was also characterized by longer time interval from diagnosis than other clinical events (149±16 versus 58±44 months, p=0.014).
Conclusions SVAR and IE, rather than AR progression, were main causes of late OHS in adult patients with sVSD and watchful waiting with close monitoring of patients with high risk echocardiographic features can be a rational option.
|