Background
Long term right ventricular(RV) apical pacing can lead to a decrease in left ventricular function(LV) and the development of heart failure. QRS width in relation to RV apical pacing is known as a predictor of LV dysfunction in patients with permanent pacemaker. The QRS width could be possiblly associated with the anatomical position in RV apex in relation to septal wall. The purpose of this study was to evaluate the relation of RV apical lead position and long-term LV systolic function.
Methods
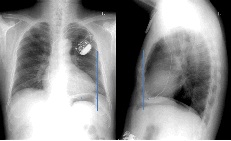
108 consecutive patients with normal LV function in baseline echocardiography who underwent permanent pacemaker implantation for advanced AV block were enrolled retrospectively. The distance of right ventricular lead to apex were measured in chest radiologic postero-anterior and lateral view (Fig.1). Baseline and long-term follow-up echocardiographic data were reviewed. All patients were divided into 2 groups as patients with preserved LV function (Group 1) and decreased LV function with ejection fraction(EF) below 50% in follow-up echocardiography.
Results
There were no differences in EF between group 1 (n=89/62.4YO) and group 2 (n=19/59.6YO). Follow-up EF was 61.8±7.40% in group 1 and 42.2±9.91% in group 2. There was no difference of the distance from apex to RV lead in chest lateral view between 2 groups (Group1 ; 2.29±1.35cm vs Group2 ; 2.27±2.72cm, p=0.946) In group 2, The distance from apex to RV lead in chest radiologic PA view showed longer distance as compared to group 1. (group1 ; 4.64±1.31cm vs group2 ; 6.05±5.92 cm, p=0.318), but there was no statistical significance between 2 groups.
Conclusions
In this study, the radiologic parameter of RV lead position in relation to apex could not predict the development of LV dysfunction. Therefore, the physiologic location with narrowest QRS width could be more important in performing RV apical pacing.
|