 Intervention of the Month Intervention of the Month |
|
| A Successful Percutaneous Coronary Intervention in Latecomer with Non-ST Elevation Myocardial Infarction |
Min Suk Kim, MD, Kye Hun Kim, MD, PhD, Ju Han Kim, MD, PhD and Myung Ho Jeong, MD, PhD, FACC, FAHA, FESC, FSCAI
The Heart Center of Chonnam National University Hospital, Gwangju, Korea
|
|
A 62-year-old male patient visited our hospital emergency department with ongoing chest pain for more than 12 hours. He had no past history of hypertension, diabetes mellitus, and dyslipidemia. He was a social drinker, and heavy smoker with 60 pack-years. Physical examination revealed no abnormal murmur or irregular beat on heart sound. He showed normal sinus rhythm with Q-wave in V1-2, and T-wave inversion in V1-4 on electrocardiogram (ECG) (Fig. 1). All cardiac enzymes were elevated with troponin-I (11.12 ng/mL), myoglobin (237 ng/mL), CK-MB (176.0 U/L), and creatine kinase (1030 U/L). So we diagnosed non-ST elevation myocardial infarction (NSTEMI), and coronary angiography (CAG) room was available, this patient underwent percutaneous coronary intervention (PCI) immediately.
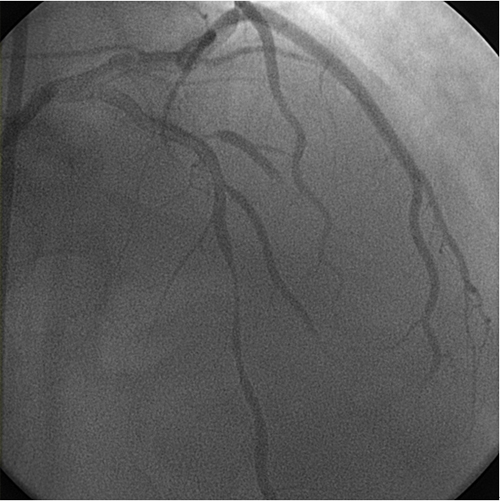
CAG via the right femoral artery revealed total occlusion of the proximal left anterior descending artery (LAD) at ostium with good collaterals from right coronary artery (RCA) (C, 100%, 0) (Fig. 2). Under bilateral guidance, wiring was done using a guidewire and a microcatheter, followed by PTCA using a 1.5 and a 2.5 mm balloon (RS:60%) and stenting using a 3.0*23 mm Xience Prime at 10 atm (Fig. 3). A repeat CAG showed no-reflow with huge amount of thrombus compromising flow in D1 branch (Fig. 4). Intra-coronary (IC) adenosine, nicorandil, clotinab were given and another stent (3.0*12 mm Xience Prime) was implanted dist to the prox LAD with overlapping at 10 atm (Fig. 5). The final CAG showed TIMI II antegrade flow without residual stenosis and slightly improved flow in D1 flow (Fig. 6). After uneventful recovery, he was discharged with anti-platelet therapy and educated smoking cessation, and has been followed up at the outpatient clinic.
The clinical benefit of PCI is controversial in stable patients with acute myocardial infarction presenting 12 hours after the symptom onset. 2010 American Heart Association (AHA) guidelines or 2009 European Society of Cardiology (ESC) guidelines recommend not to perform PCI in stable latecomers. But, in some recent studies reported that PCI in stable latecomer can be beneficial in long-term clinical outcomes. In stable patients with STEMI presenting 12 to 72 hours after symptom-onset, PCI was associated with significant improvement in 12-month clinical outcome in Korea Acute Myocardial Infarction Registry (KAMIR). But the optimal timing of PCI requires more stuides.
|
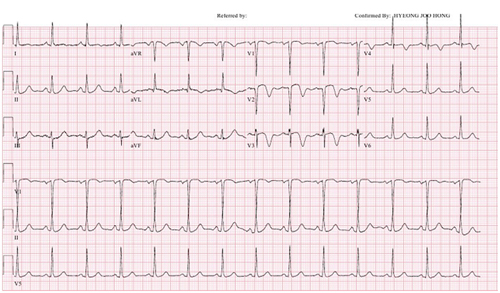 |
▲ Figure 1. ECG showed normal sinus rhythm with Q-wave in V1-2, and T-wave inversion.
|
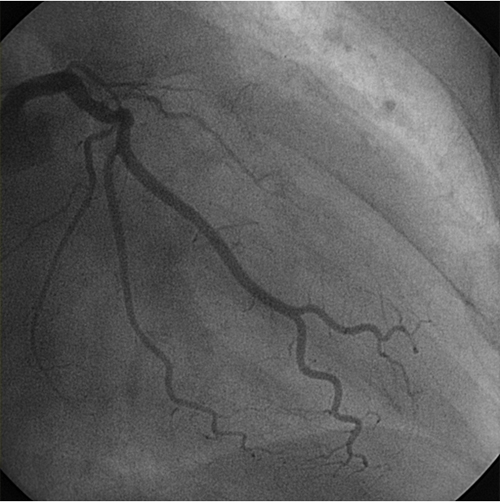 |
▲ Figure 2. CAG via the right femoral artery revealed total occlusion of the proximal LAD at ostium with good collaterals from RCA.
|
 |
▲ Figure 3. Wiring was done using a guidewire and a microcatheter, followed by PTCA using a 1.5 and a 2.5 mm balloon (RS:60%) and stenting using a 3.0*23 mm Xience Prime at 10 atm .
|
 |
▲ Figure 4. A repeat CAG showed no-reflow with huge amount of thrombus compromising flow in D1 branch.
|
 |
▲ Figure 5. Intra-coronary (IC) adenosine, nicorandil, clotinab were given and another stent (3.0*12 mm Xience Prime) was implanted dist to the prox LAD with overlapping at 10 atm.
|
 |
▲ Figure 6. The final CAG showed TIMI II antegrade flow without residual stenosis and slightly improved flow in D1 flow.
|
|
| |
위의 이달의 중재술을 보신 선생님들의 의견을 아래의 의견 쓰기에 의견을 남겨 주십시오.
선생님들의 다양한 의견을 받습니다.
|
![[의견쓰기]](/image/comment_btn.gif) |
Warning: include(/home/virtual/circulationadmin/new/info/comment_index.php) [function.include]: failed to open stream: No such file or directory in /home/virtual/circulationadmin/new/info/case/201203/case201203.htm on line 178
Warning: include() [function.include]: Failed opening '/home/virtual/circulationadmin/new/info/comment_index.php' for inclusion (include_path='.:/usr/local/php/lib/php') in /home/virtual/circulationadmin/new/info/case/201203/case201203.htm on line 178
|
|
|