 Intervention of the Month Intervention of the Month |
|
| A Case With Successfully Diagnosed As Exercise Induced Variant Angina |
|
Jong Hyun Yoo, MD, Min Goo Lee, MD, Keun-Ho Park, MD, Doo Sun Sim, MD, PhD, Young Joon Hong, MD, PhD, Ju Han Kim, MD, PhD, YoungkeunAhn, MD, PhD, FACC, FSCAI and Myung Ho Jeong MD, PhD, FACC, FAHA, FESC, FSCAI
|
|
A 54-year-old male patient visited Chonnam National University Hospital (CNUH) with chest pain aggravated while exercise for1 years. The pain was developed when he walked about 30 to 40 meters on flatland. He underwent treadmill exercise test at CNUH 8 months ago. The electrocardiography (ECG) during treadmill test showed significant ST segment changes of 2mm depression in II, III, aVF and V3-6 (Figure 1). He had no past history of hypertension, diabetes mellitus, and familial history of coronary artery disease. But he had dyslipidemia.He was a social drinker and ex-smoker with 40 pack-years.Physical examination revealed no abnormal murmur or irregular beat on heart sound. He showed normal sinus rhythm on ECG. Cardiac enzymes were not elevated with troponin-I (0.01ng/mL) and CK-MB (1.30 U/L). So we diagnosed as effort angina tentatively. Then we described medicines for effort angina for 8 months, but his exertional chest pain was not relieved. At last we decided to perform coronary angiography (CAG) to evaluate coronary arterial abnormality like stenosis.
His CAG showed nosignificant stenosis in both coronary arteries (Figure 2). We decided to do CAG with ergonovine provocation test to rule out variant angina, and Myocardial Single Photon Emission Computed Tomography (M-SPECT) to evaluate myocardial ischemia by pharmacologic stress. So we stopped to give calcium channel blocker (CCB) and nitrate to him. The next day echocardiography was done. It showed normal chamber size with normal wall thickness, and good left ventricular systolic function without regional wall motion abnormality. M-SPECT using adenosine showed moderate sized, reversible perfusion defect in mid to basal inferior wall. It meant endocardial damage in mid to basal inferior wall (Figure 3). We performed CAG with ergonovine provocation test. When we injected 3rd dose of intra-coronary (IC) ergonovine, significant spasm was provoked in left coronary artery, especially for proximal left anterior descending (LAD) artery, and the patient complained of chest pain with which he was familiar. All spasm and his chest pain were relieved after IC nitroglycerin (Figure 4). CAG with ergonovine provocation test showed ergonovine induced significant spasm in left coronary artery, so we could diagnosed as variant angina. But he complained chest pain only when he got exercise. Then we decided to perform exercise stress M-SPECT to diagnose exercise induced variant angina. Exercise stress M-SPECT was taken after treadmill exercise by modified Bruce protocol. Exercise stress test showed small sized, mild reversible perfusion defect in apico and mid anterior wall (Figure 5). So we could know he had exercise induced anterior wall ischemia, and diagnosed as exercise induced variant angina. At discharge, the patient did not complain of chest discomfort. He was prescribed CCB, nitrate, statin daily.
The patient had typical effort angina and positive result of treadmill test, but no coronary stenosis and negative finding of M-SPECT using adenosine. So we performed CAG with ergonovine provocation test and M-SPECT after exercise to diagnose exercise induced variant angina. CAG with ergonovine provocation test and M-SPECT after exercise showed the result compatible with exercise induced variant angina. The definition, diagnostic criteria, and management of exercise induced variant angina were not established. There are few published articles about it nowadays. So we introduced the case diagnosed as exercise induced variant angina using CAG with ergonovine provocation test and exercise stress M-SPECT.
|
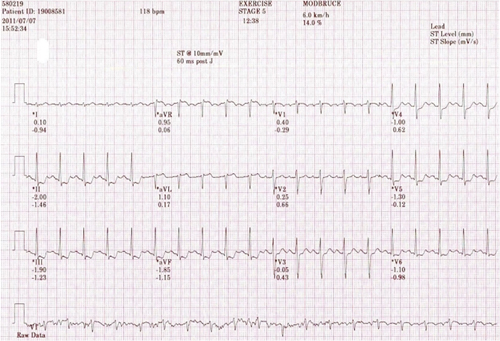 |
▲ Figure 1. Exercise stress electrocardiography (ECG). ECG showed ST depression in II, III, aVF, V3-6 at stage 5 of treadmill test by modified Bruce protocol.
|
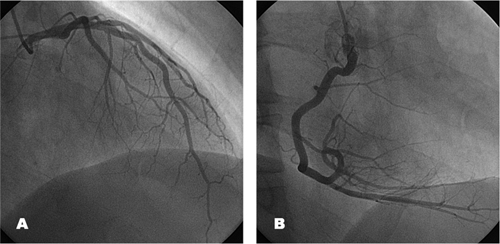 |
▲ Figure 2. . Coronary angiography. No significant stenosis in left coronary artery (A) and right coronary artery (B).
|
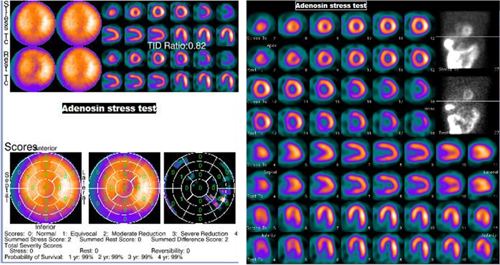 |
▲ Figure 3. Myocardial Single Photon Emission Computed Tomography (M-SPECT) with adenosine stress test. M-SPECT showed moderate sized, reversible perfusion defect in mid to basal inferior wall.
|
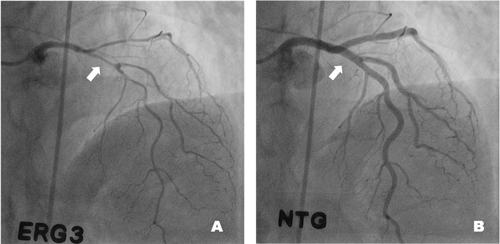 |
▲ Figure 4. Coronary angiography with Ergonovine (ERG) stress test. Intra-coronary (IC) ERG provoked significant spasm in left coronary artery, especially for proximal left anterior descending artery (white arrow, A). All spasm was relieved completely after IC nitroglycerin (B).
|
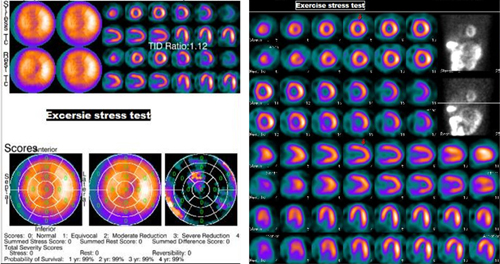 |
▲ Figure 5. Myocardial Single Photon Emission Computed Tomography (M-SPECT) with exercise stress test. M-SPECT showed small sized, mild reversible perfusion defect in apico and mid anterior wall.
|
|
| |
위의 이달의 중재술을 보신 선생님들의 의견을 아래의 의견 쓰기에 의견을 남겨 주십시오.
선생님들의 다양한 의견을 받습니다.
|
![[의견쓰기]](/image/comment_btn.gif) |
Warning: include(/home/virtual/circulationadmin/new/info/comment_index.php) [function.include]: failed to open stream: No such file or directory in /home/virtual/circulationadmin/new/info/case/201205/case201205.htm on line 170
Warning: include() [function.include]: Failed opening '/home/virtual/circulationadmin/new/info/comment_index.php' for inclusion (include_path='.:/usr/local/php/lib/php') in /home/virtual/circulationadmin/new/info/case/201205/case201205.htm on line 170
|
|
|