CASE
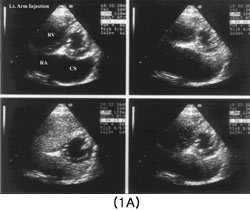
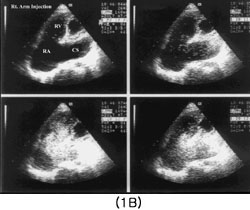
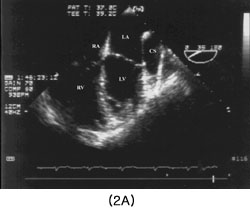
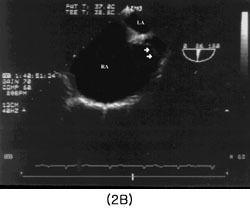
A 39 year old women was admitted to the hospital for the evaluation of cardiomegaly on chest radiograph. Except for intermittent palpitation for several years, she felt no symptom and denied any history of heart diseases. Physical examination revealed mild increase of jugular venous pressure and mild hepatomegaly. A grade III/VI holosystolic murmur was heard over the left lower sternal border. Her ECG demonstrated wandering atrial pacemaker and simple chest x-ray showed a moderate cardiomegaly. A transthoracic echocardiographic examination(TTE) revealed enlarged right atrium(RA), right ventricle (RV) and huge coronary sinus(CS) along the posterior side of left ventricle. Coaptation failure of tricuspid valve leaflets caused severe tricuspid regurgitation on Doppler examination although there was no morphologic abnormality of tricuspid valve leaflets. Since markedly enlarged CS is unusual in persistent left SVC, we performed TTE with contrast enhancement by intravenous injection of agitated saline from both arms. Echo contrast appeared CS in first, and RA, RV in sequence regardless of injection sites (figure 1A and 1B). Multiplane transesophageal echocardiographic examination(TEE) revealed huge CS(figure 2A) connected into right atrium and a blind pouch(figure 2B) where right SVC should be connected in normal heart. TEE with repeated injection of agitated saline from both arms again demonstrated that echo contrast filled in the same sequence as TTE. Cardiac MRI was performed to rule out any other associated anomaly and no other cardiac or vascular abnormalities were observed.
DISCUSSION
Absent right SVC with persistent left SVC draining into dilated CS, first described in 1862(3), is a rare anomaly of systemic venous return. The accurate incidence of this anomaly is unknown. Pugliese et al. Reported 6 cases from 4,100 patients who had cardiac catheterization for congenital heart diseases with normocardia(4). The clinical presentation and the indication for operation vary depending on the associated cardiac anomalies(5). In the routine examination, simple chest x-ray may show a cardiomegaly or contour abnormality of the left superior mediastinum. ECG may show a leftward deviation of the P axis or arrhythmia. The diagnosis of this anomaly and the associated other cardiac malformations have usually been made by the CT and MRI. TTE with contrast was used for the diagnosis in a case report(6).
REFERENCES
1. Rusk RA, Bexton RS, McComb JM. Persistent left sided and absent right sided superior vena cava complicating permanent pacemaker. Heart 1996; 75:413
2. Lenox CC, Zuberbuhler JR, Park SC, et al. Absent right superior vena cava with persistent left superior vena cava; Implication and management. Am J Cardiol 1980; 45:117-22
3. Karnegis JW, Wang Y, Winchekk P, Edwards JE. Persistnet left superior vena cava, fibrous remnant of the right superior vena cava and ventricular septal defect. Am J Cardiol. 1964; 14:573-7
4. Pugliese P, Murzi B, Aliboni M, Eufrate S. Absent right superior vena cava and persistent left superior vena cava; clinical and surgical considerations. J Cardiovascular Surg. 1984; 25:134-7
5. Mazzucco A, Bortolotti U, Stellin G, Gallucci V. Anomalies of the systemic venous return; A review. J of Cardiac Surgery. 1990; 5:122-33
6. Oguni H, Hatano T, Yamada T etal. A case of absent right superior vena cava with persistent left superior vena cava: cross-sectional echocardiographic diagnosis. Heart & Vassels 1985; 1:239-43
FIGURE LEGENDS