Proteoglycan Is A Major Component of Recurrent Coronary Stent Restenosis
Bora Yang, MD and Myung Ho Jeong, MD
The Heart Center, Chonnam National University Hospital, Gwangju, Korea
ABSTRACT
A percutaneous coronary intervention (PCI) is known to be one of effective methods in treatment of coronary artery disease. However, restenosis remains as a major limitation of PCI. Although neointimal cell proliferation is suspected to be the major cause of this problem, few histological characterization of recurrent instent restenosis exist.
We report a case of 61-year-old man suffered from unstable angina due to second coronary instent restenosis in proximal left anterior descending artery (LAD). An atherectomized tissue obtained by directional coronary atherectomy showed myxoid tissue characterized by few stellate smooth muscle cells in the abundant extracellular matrix, which was blue-colored proteoglycan in modified Movat staining. Thus the major component of recurrent coronary instent restenosis is proteoglycan.
(A) (B)
Fig 1. A follow-up coronary angiogram revealed critical restenosis in the proximal left anterior descending artery (A) and successful percutaneous coronary intervention using balloon was performed (B).
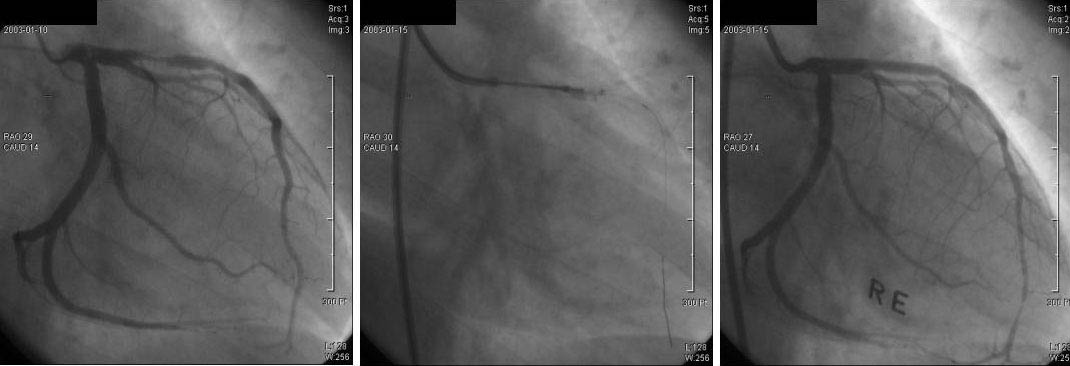
(A) (B) (C)
Fig 2. A follow-up angiogram at 6 months after ballooning for stent restenosis revealed second in-stent restenosis in the proximal left anterior descending coronary artery (A) and directional atherectomy was performed for the second in-stent restenosis (B). A vascular brachytherapy was performed using Re-188 filled balloon (C).
(A) (B)
Fig. 3. An atherectomized tissues of coronary in-stent restenosis. Hematoxyllin & Eosin stain (´ 200) shows myxoid tissue characterized by stellate smooth muscle cells in the loose extracellular matrix (A). In modified Movat staining, blue colored proteoglycan is shown as a major component in this myxoid tissue. Yellow colored collagen is intermingled with proteoglyans.
 에 글을 써주시기 바랍니다
에 글을 써주시기 바랍니다