|
 Image of the Month Image of the Month |
|
|
|

|
|
▷ Case (2003. 02)
|
|
 Case Case
|
A 49 year old man was referred for palpitation and dizziness, which were not associated with exertion. He had felt chest fluttering all the time during ordinary activity for recent 6 months. Physical examination revealed intermittently irregular and rapid heart rate. Nothing was significant on cardiac auscultation.
ECG showed normal sinus rhythm with intermittently noted atrial arrhythmia and incomplete right bundle branch block (Fig 1). Holter ECG showed frequent non-sustained atrial tachycardia, accompanied by palpitation (Fig 2). Echocardiography showed no remarkable findings.
Electrophysiology study showed that the earliest activation during atrial tachycardia was from the left side atrium. After trans-septal puncture, 3-D noncontact mapping catheter (Ensite 3000 system) was positioned at the left atrium. This system permits generation of a potential map from a single premature complex and helps guide difficult ablation procedure. Mapping consistently showed the origin of atrial tachycardia from right inferior pulmonary vein (RIPV) ostium (movie 1). Radiofrequency energy was delivered at the RIPV ostium to disconnect PV from the LA (movie 2). After ablation, atrial tachycardia was no longer induced with isoproterenol infusion and rapid atrial pacing.
Patient remained free of arrhythmia recurrence during a follow-up for 6 months. Holter ECG showed neither tachycardia nor sinus pause (fig 3).
|
|
|
Legend
|
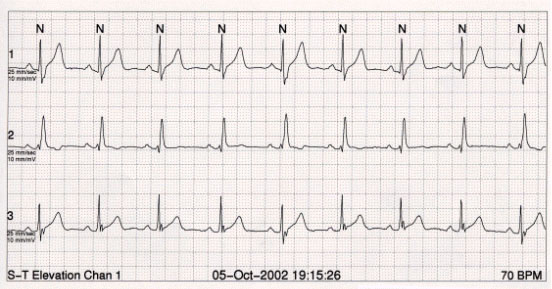
Figure 1.
Standard 12-lead ECG showed normal sinus rhythm with marked sinus arrhythmia and incomplete right bundle branch block..
|
 |
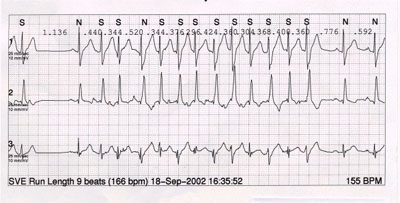
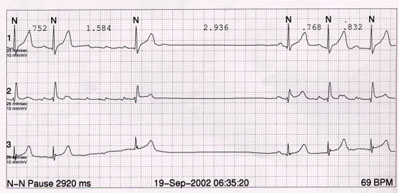
Figure 2.
Holter ECG showed frequent episodes of non-sustained atrial tachycardia accompanied by frequent sinus pause.
|
|
Movie 1. [view]

This movie showed that one beat of sinus rhythm was followed by consecutive atrial tachycardia. 3-D non-contact mapping system (Ensite 3000) consistently showed repetitive focal electrical activity originated from RIPV (right inferior pulmonary vein) os. Note that the morphology of atrial electrogram at virtual lead (24) during sinus rhythm differs from that of atrial tachycardia.
|
Movie 2. [view]

This movie revealed that after multiple applications of RF to RIPV ostium. The entrance block from the left atrium to RIPV was noted, which was validated by proximal coronary sinus pacing.
|
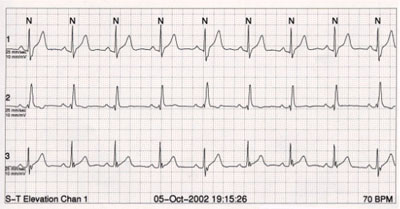
Figure 3.
Holter ECG after catheter ablation showed normal sinus rhythm without a single atrial premature complex.
|
 |
|
provided by 안암병원 순환기내과 박상원 김영훈
☞ 질문이나 의견이 있으시면 회원들의 공간
 에 글을 써주시기 바랍니다 에 글을 써주시기 바랍니다
|
▲Top
|
|